
{kind=link}
The Vaccine Adverse Events Reporting System (VAERS) is a database run jointly by the Centers for Disease Control and Prevention and the Food and Drug Administration for reporting vaccine injuries whose major strength is the same as its major weakness. The major strength of VAERS is that anybody—and I do mean anybody—can report a suspected vaccine injury to it. You don’t have to be a physician or other health care provider to report a suspected vaccine injury, and, given what VAERS was designed for, that’s a good thing. That’s because VAERS was designed as an early warning system, a “canary in the coal mine,” if you will, to detect potential adverse events (AEs) from new and existing vaccines. What that design means, though, is that VAERS inherently cannot be used to accurately estimate the incidence or prevalence of specific injuries due to specific vaccines, because it is a passive surveillance system that relies on voluntary reporting. The idea is that VAERS is a hypothesis-generating, not a hypothesis-testing, system, because, given that anyone can report anything to VAERS, factors other than incidence or prevalence can hugely impact reporting to VAERS. VAERS is thus subject to the base rate fallacy, which occurs when cases or raw numbers of a phenomenon are examined without statistically correct consideration of the base rate or prior probability of that phenomenon being observed. That’s why any hypothesis generated by VAERS must be tested against more rigorous systems like the Vaccine Safety Datalink (VSD), the Clinical Immunization Safety Assessment (CISA) project, or FDA’s Post-licensure Rapid Immunization Safety Monitoring System (PRISM), active reporting systems that actively monitor electronic health records for AEs after vaccination in order to identify potential signals. Usually the VSD is the database most commonly used to investigate safety signals found in VAERS.
Indeed, that’s why the greatest weakness of VAERS is that anybody can report anything to it. As we have discussed here time and time again, the main problem with using VAERS to estimate the frequency of AEs after vaccination is precisely that, in essence, anyone with access to the Internet, mail, or the telephone can report anything to VAERS, as was demonstrated by bloggers years and years ago when one autism advocate filed a report claiming that the flu vaccine had turned him into The Incredible Hulk and another claimed a vaccine had turned his daughter into Wonder Woman. Both reports were accepted. In fairness, ultimately someone from VAERS did contact these people to ask about the reports, and the reports were removed. However, had they refused, reports that vaccines might turn one into the Hulk or Wonder Woman might still be in the database. Another example that I like to cite is how in the 1990s and beyond, lawyers suing vaccine manufacturers for vaccine-induced autism (which is not a thing, given that the evidence overwhelmingly shows that vaccines do not increase the risk of autism) gamed VAERS by encouraging potential litigants to report their children’s autism to VAERS as a vaccine-related AE, as I first discussed in 2006. (Yes, you read that right! 2006! VAERS has been a favorite tool of antivaxxers to mine for deceptive associations going back at least two decades.)
Interestingly, the greatest weakness in VAERS, namely reporting biases and how much changes in reporting that can be affected by news, government campaigns to encourage reporting (e.g., the way the CDC gave instructions to vaccinees receiving COVID-19 vaccines on how to report to VAERS), misinformation, news reports, and disinformation, can also make it a source for preliminary research on factors that can affect the reporting of vaccine-related AEs to VAERS. This aspect of VAERS was in evidence in a study published a week and a half ago in JAMA Open Network, the open-access peer-reviewed journal run by JAMA. The study, by a group of investigators from the University of Pennsylvania and Washington University, was entitled Reports of COVID-19 Vaccine Adverse Events in Predominantly Republican vs Democratic States. Its findings made the news (of course) because they were rather provocative, albeit not unexpected, given how far to the right the political center of gravity of the antivaccine movement has shifted over the last 15 years, particularly during the pandemic. I’ll get into the details in a moment, including weaknesses of the study, but, in brief, examining 620,456 vaccine AEs reported to VAERS from adults 18 and older, investigators found that “the more states were inclined to vote Republican, the more likely their vaccine recipients or their clinicians reported COVID-19 vaccine AEs.”
Unsurprisingly, the study briefly made the news and the rounds on Easter weekend after it was published, although to me the news coverage was actually not very intense and relatively mild, with the few articles I saw about the study having bland titles like Reports of COVID-19 Vaccine Adverse Events in Predominantly Republican vs Democratic States and People in Republican-voting states more likely to report Covid-19 vaccine side effects, study says. It was apparently the news stories like these that drew the attention of someone whose bad COVID-19 takes have been a fairly frequent topic of this blog, Dr. Vinay Prasad, who took to his paid Substack to complain, Unhelpful, inflammatory Jama Network Open paper suggests that people in Red states dream up vaccine injuries and mixed in with a discussion of weaknesses of the study acknowledged by the authors a claim so utterly divorced from reality that it reminded me of a catchphrase that a certain YouTuber employs at some point in all his videos to comic effect, only with Dr. Prasad seemingly using it seriously.
Before I discuss the study and Dr. Prasad’s reaction to it, I will note that nowhere does Dr. Prasad take note of a different kind of reaction to it coming from antivaxxers, reactions from antivaxxers like Covid Vax Deaths Surge in Republican-Voting States, Study Finds, proclaiming. No, that’s not what this study found. It’s what the authors write in the introduction as part of their rationale for doing the study:
COVID-19 mortality has been higher in US jurisdictions that are more conservative in their party registration,1 voting history,2 or representation.3 These differences are likely explained, in part, by differences in vaccination rates. Counties voting for former President Donald Trump in the 2020 presidential election had substantially lower COVID-19 vaccination rates than counties voting for President Joe Biden.4,5
None of this is particularly controversial, but Dr. Prasad has apparently decided to echo antivax takes on this study:
Note the use of the phrase “dreamed up.” Nowhere in the study is it claimed that people in red states “dream up” vaccine injuries. I also note that antivaxxer Dr. Paul Alexander is very much impressed with Dr. Prasad’s take on the study, which is never a good sign if you think you are science-based, as Dr. Prasad does.
Let’s take a look at the study itself, which is fairly simple in design. Afterwards, we’ll look at Dr. Prasad’s mix of reasonable critiques with unreasonable critiques, to see what form of negative spin he puts on it.
Red, Blue, and VAERS
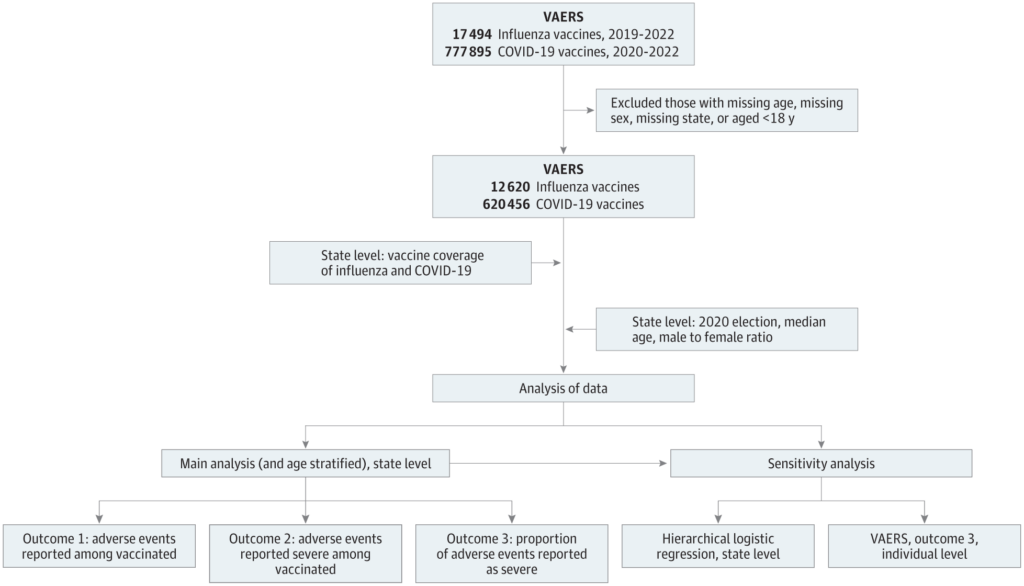
Getting back to the study, it’s of a fairly simple design. In brief, it is a cross-sectional study of reports to the VAERS database for injuries after COVID-19 vaccination that identified total of 620 456 AE reports (mean [SD] age of vaccine recipients, 51.8 [17.6] years; 435 797 reports from women [70.2%]; a vaccine recipient could potentially file more than one report, so reports are not necessarily from unique individuals) for COVID-19 vaccination. The time period examined was from 2020 to 2022, and the study looked at adults 18 years of age and older. As a control, the authors examined VAERS reports for injuries due to influenza vaccines. The results were broken down by state, with each state’s reporting of AEs after COVID-19 vaccination and after influenza vaccination (from 2019 to 2022) compared to the state’s voting record in the 2020 Presidential election, specifically the percentage of vote that went for the Republican candidate Donald Trump. These outcomes were then examined:
We separately examined 3 different outcomes: (1) rates of any AE among vaccine recipients, (2) rates of any severe AE among vaccine recipients, and (3) the proportion of AEs reported as severe. To account for baseline variation in VAERS reporting behavior across states, we also used each state’s AE reporting rate for the influenza vaccine (Figure 1).
As the authors put it in the introduction, they were using a major weakness of VAERS as a strength for purposes of their study:
However, what is a weakness in the VAERS in systematically capturing AEs is a strength in quantifying the perception of AEs and the motivation to report them. Without a plausible reason to believe that vaccine recipients and their clinicians in Republican-inclined states will objectively encounter different rates of vaccine AEs than those in Democrat-inclined states, or have different abilities to report them, differences in reporting of those AEs will reflect the product of how those AEs are perceived and the inclination to report them, either by the vaccine recipients or their clinicians.
In fairness, one might reasonably question whether there are objective reasons why people in red states might objectively encounter different rates of AEs after vaccination, but that isn’t really what Dr. Prasad does in his critique, as you will see. That quibble aside, the authors made adjustments for the male-female ratio and median age to “adjust for state-level heterogeneity in VAERS reporting unconnected to COVID-19 vaccination.” They also did a number of sensitivity analyses, to determine how robust their model was was and identify potential confounders:
In sensitivity analyses, we (1) stratified regressions by age groups or excluded the District of Columbia; (2) used hierarchical logistic regression with state-specific random effects as another approach to account for heterogeneity in the baseline VAERS reporting rate; (3) performed an individual-level analysis for the proportion of AEs reported as severe within VAERS reports, adjusting for individual age, sex, and history of medication or allergy; and (4) relaxed assumptions of linearity by using locally estimated scatterplot smoothing.10
The flowchart looked like this:
The results were quite striking:
We observed 620 456 AE reports (435 797 from women [70.2%]; mean [SD] age, 51.8 [17.7] years) associated with COVID-19 vaccination (Table 1). A vaccine recipient could potentially file more than 1 report, so reports are not necessarily from unique individuals. A 10% increase in state-level Republican voting was associated with increased odds of AE reports (odds ratio [OR], 1.05; 95% CI, 1.05-1.05; P < .001), severe AE reports (OR, 1.25; 95% CI, 1.24-1.26; P < .001), and the proportion of AEs reported as severe (OR, 1.21; 95% CI, 1.20-1.22; P < .001) (Table 2). These positive associations between political inclination and reports of COVID-19 vaccination AEs are shown in Figure 2 against no associations between political inclination and reports of influenza AEs. These findings were seen across all age strata in stratified analyses and in analyses excluding the District of Columbia (Table 2) and were sustained in sensitivity analyses (eTable 2 and the eFigure in Supplement 1; Figure 3).
Graphically, the results looked like this:
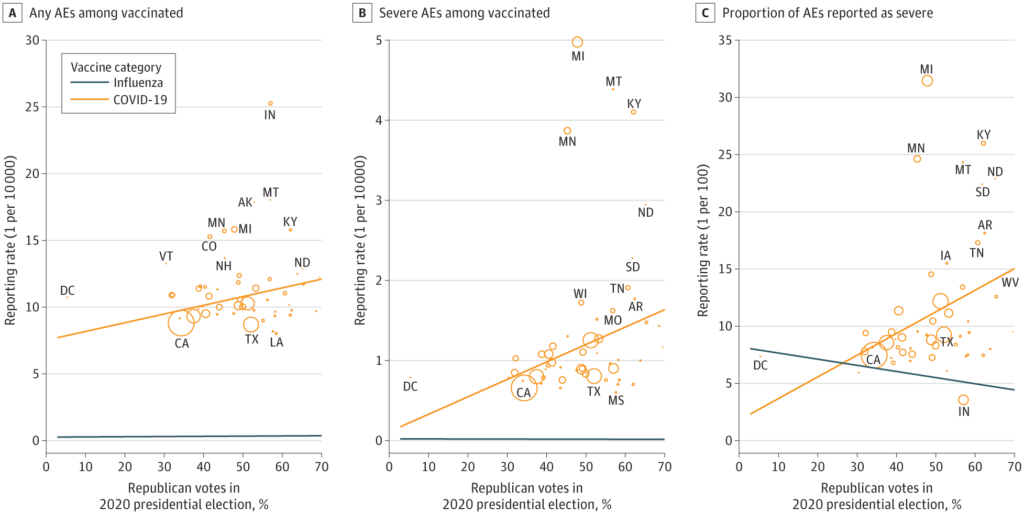
All these differences are rather striking, particularly the reports of severe AEs. Overall, the authors estimated, a 10% increase in state Republican voting was associated with a 5% increase in the odds that a COVID-19 vaccine AE would be reported to VAERS, a 25% increase in the odds that a severe AE would be reported, and a 21% increase in the odds that any reported AE would be severe.
Sensitivity analyses carried out to try to exclude other factors that might confound the analysis found that…
…individuals with other vaccines or history of medication or allergy do not show a significant association with political inclination, male recipients of the COVID-19 vaccine show a similar association with political inclination as female recipients, and older recipients of the COVID-19 vaccine show a stronger association with political inclination.
The results led the investigators to conclude:
This study found that the more states were inclined to vote Republican in the 2020 US presidential election, the more likely their vaccine recipients or clinicians were to report COVID-19 vaccine AEs. This association between political inclination and vaccine AE reporting was not seen for the influenza vaccine. The results are consistent with a relative overreporting of vaccine AEs among Republicans or a relative underreporting among Democrats.
Further noting:
The association between observation and belief runs both ways. The adage “seeing is believing” recognizes that our individual experiences inform our sense of truth, and “believing is seeing” recognizes that our preconceptions modulate what we experience in the first place. In finding that Republican-inclined states show higher COVID-19 AE reporting than Democrat-inclined states, this study suggests that Republicans are more likely to perceive or report those AEs and that Democrats are less likely to.
All of this is, of course, not unreasonable. Because VAERS is a passive reporting database, that means that what it is recording are AEs that the people reporting the AEs perceive as having been likely due to the vaccine. One only has to point to examples of people claiming that sudden cardiac deaths were due to COVID-19 vaccines, even when they occur weeks, months, or years after vaccination, to emphasize the point that perception affects reporting to VAERS. The same thing is true of cancer, with antivaxxers perceiving nearly any case of cancer occurring after vaccination with COVID-19 vaccines, be it days, weeks, months, or even a year later when the cancer is diagnosed, as being “turbo cancers” caused by the vaccines. If deaths and cancer can be incorrectly perceived as due to the vaccines, then of course lesser AEs will be even easier to have been incorrectly attributed to vaccines. Again, as the authors point out, this goes both ways. If you believe the vaccines are safe and effective, you might be less likely to attribute something that might be a real vaccine injury to the vaccines, a point that antivaxxers offended by this study miss.
The Prasad is outraged
Of course, nuance has never been Dr. Vinay Prasad’s strong suit, at least not when there is an audience to enrage and clicks to be had. He is outraged that this study found what it found:
How to rebuild trust? By doubling down on petty partisan politics, according to a new JAMA NO paper.
And then:
The article claims that people in Red states report more vaccine injuries than people in Blue states. It concludes that either Republicans are more likely to “perceive” injuries, or Dems less likely.
I’m not sure how this finding is “doubling down” on petty partisan politics. It seems that Dr. Prasad is more outraged by a single example of news coverage of the study in which Dr. Eric Topol in a STAT+ article:

Note how the text fades out. Dr. Prasad apparently doesn’t have a subscription to STAT+ and therefore didn’t read the whole article, which might or might not have included more from Dr. Topol. Unfortunately, neither do I; so I can’t check. However, I must agree that Dr. Topol’s not wrong in that, again, the political center of gravity of the antivaccine movement has shifted far to the right over the last decade, especially since the pandemic; moreover, we know that vaccine hesitancy and resistance tend to be higher in states with a high proportion of Republicans. Heck, economist turned incompetent antivax “epidemiologist,” Michigan State University Professor Mark Skidmore inadvertently found data suggesting, for instance, that political orientation greatly affects whether a person perceives a death as having been due to COVID-19 vaccines or not. Too bad he was so hellbent on deceptively spinning his survey data into “proving” that COVID-19 vaccines have killed hundreds of thousands of Americans.
Let’s get to the substance, such as it is, of Dr. Prasad’s criticism:
Let me explain why this is a poor choice. The factors that predict whether someone has an adverse event to influenza vaccine may not be the same as those that predict adverse events from covid shots. It could be that there are actually more covid vaccine injuries in one group than another— even though both had equal rates of influenza injuries.
Yes, but that’s not why the authors were using influenza vaccines as a control. They clearly thought that political orientation would have much less of an effect on whether a person perceived an AE as having been due to the vaccine than it would for COVID-19 vaccines. After all, flu vaccines have been around a long time, and most people, aside from antivaxxers and the vaccine-hesitant, view them rather benignly, or at least not with fear and loathing, based on messaging that is more prevalent on one side of the political spectrum than the other. Of course, Dr. Prasad likely knows this, but that doesn’t stop him from spinning a fantastical confounder with a dubious comparison:
Another way to think of it is, there can be two groups of people and you can balance them by the rate with which they get headaches from drinking wine, but one group can be more likely to get headaches from reading without glasses because more people in that group wear glasses. In other words, states with more republicans might be states with specific co-morbidities that predict COVID vaccine adverse side effects but not influenza vaccine side effects. We already know that COVID vaccine injuries do affect different groups (young men, for e.g.).
I note that the only example that Dr. Prasad can cite (young men being more likely to experience myocarditis after COVID-19 vaccination) would have likely shown up in the sensitivity analyses based on age and gender. It didn’t. Absent that, all Dr. Prasad is doing is coming up with a hypothetical confounder that he can’t prove. After all, if he could, he would have cited specific conditions or demographic traits of different states—other than being young and male—that might have confounded these results.
Next up:
These data are ecological. It doesn’t prove that republicans themselves are more likely to report vaccine injuries. It would not be difficult to pair voting records with vaccine records at an individual patient level if the authors wished to do it right— another example of research laziness.
It is correct that this study is ecological and that ecological studies can find associations that don’t hold up to more rigorous analysis. The authors are very upfront about that, stating that it is one of the study’s weaknesses but also explaining why they think that the ecological design of the study was unlikely in this case to have produced a false positive correlation:
This study is limited by its ecological design.12 Both vaccine reporting and political voting occur at the level of individuals, but here they are measured at the level of states. Nevertheless, the only way the results might not support a relatively increased AE reporting rate among individual Republican-voting citizens is if Republican-voting citizens were less likely to report but far more likely than Democrat-voting citizens to be vaccinated in the first place or if, as the proportion of Republican-voting citizens in a state increased, the AE reporting rates among the progressively fewer Democrat-voting citizens increased at an even steeper rate. Neither possibility seems likely.
In particular, that latter explanation appears very unlikely.
Remember, though, how I referred to a catchphrase of a certain YouTuber whose videos I like? The part where Dr. Prasad blithely says that it “would not be difficult to pair voting records with vaccine records at an individual patient level if the authors wished to do it right— another example of research laziness” is what brought to mind that catchphrase about how “difficult” this task might be, because apparently Dr. Prasad thinks that it would be “super easy, barely an inconvenience.” By way of background, that catchphrase comes from YouTuber:
Super easy, barely an inconvenience is one of the main catchphrases of the series, Pitch Meetings always said by Screenwriter Guy. It is an on-running phrase used in nearly every episode whenever Studio Executive Guy thinks something would probably be difficult, to which the the guy giving the pitch responds that it would actually be “super easy, barely an inconvenience”, which pokes fun at the fact that the thing being referred to should probably be more difficult than it ends up being.
I could point to just how difficult getting institutional review board (IRB) approval for the sort of massive study that Dr. Prasad says “would not be difficult” would likely be, and I’m not even considering getting the funding to carry out such a combined epidemiological and social sciences study would be.
If you were to listen to Dr. Prasad, you’d think that pairing up voting records with over 600,000 VAERS records for COVID-19 vaccine AEs and political affiliation of individuals would be “super easy, barely an inconvenience” that only wasn’t done because the investigators who did this study were somehow too “lazy” to bothered. This is an insult to the investigators. After all, as scientists we all want to do the most rigorous studies that we can manage, but sometimes you have to do what is possible rather than ideal. This study appears to be about the best ecological study of this type that could be done, working within the realm of the feasible and what the authors likely had funding to accomplish. It’s basically the same deceptive technique that Dr. Prasad employs when he complains about there not being any randomized controlled clinical trials (RCTs) sufficiently “rigorous” for his liking. (Never mind that there is no elite RCT strike force.) It’s what I like to call methodolatry, or fundamentalist evidence-based medicine (EBM) that discounts any non-RCT as crap, regardless of ethics or feasibility of doing the desired “ideal” RCT. It’s the sort of fundamentalism that antivaxxers like RFK Jr. and his lawyer Aaron Siri have used to deceptively imply that the childhood vaccination schedule is somehow “unsafe” because not all vaccines have undergone RCTs versus a placebo control. (I discussed in great depth why this is nonsense here and described how such methodolatry and EBM fundamentalism have been weaponized against public health here.) Dr. Prasad fell for that argument on vaccines and here is doing a variation of the same thing with epidemiology, bemoaning a decent, achievable ecological study because it is not an in-depth, individual patient-record study.
It would actually be a difficult, massive undertaking. First, the VAERS report records would have to be de-anonymized, so that the investigators had names of the people making the VAERS reports. Then the authors would have to figure out who the actual patient injured was. (After all, family members, spouses, friends, and health care workers can make a report to VAERS.) They would then have to match over 600,000 names to voting records in 50 states. They’d also have to decide how they were going to assign political orientation, Democrat, Republican, or Independent, to each VAERS entry. In states in which voters have to declare a party affiliation when they register to vote, it might be fairly “easy” (but not “super easy, barely an inconvenience”). In other states, they might have to figure it out by looking at records for primary elections and seeing which ballots the people behind the VAERS entries selected. Michigan (where I am registered to vote), has an open primary and does not require one to declare a party when registering to vote. However, for any given primary election, you have to pick a Republican or Democratic primary ballot when you vote and can only vote for the primary candidates in that party. You can, however, pick the ballot for either party in any given primary, voting, for example, for Republican candidates in one primary and then the next primary picking a Democratic ballot and choosing among Democrats. For other states with open primaries it could be quite difficult to assign party affiliation to VAERS entries from the voting records, and assigning party would be impossible in states with open primaries that do not require voters to declare a party affiliation when they register to vote and allow voters to vote for both Democrats and Republicans in the primary. This latter group is pretty large.
Seriously, Dr. Prasad. WTF? “Not difficult”? Yes, in Michigan, for instance, you could find out which people reporting to VAERS chose a Republican or Democratic ballot for the Presidential primary, but it would hardly be “not difficult.” And that’s just one state. Every state has different laws and rules. Seriously, ask political scientists how “not difficult” it is to figure out the party affiliations of voters in all 50 states, and that doesn’t even count the question of people registered in one party voting in the other party’s primary in order to try to get a weaker candidate nominated.
Of course, I’m pretty sure that Dr. Prasad knows that it’s anything but “not difficult” to get access to the names of people in the VAERS AE entries, match them on an individual level to voting records in their state, and then correctly assign party affiliation to each one. I do, however, have to leave open the possibility that, as is the case when he says how “super easy, barely an inconvenience” it would be to do randomized controlled clinical trials of every little question related to COVID-19, such as masking, vaccines, social distancing, and “lockdowns.”
The bottom line
So, Dr. Prasad’s deceptive audience-captured attacks on it notwithstanding and the obstinate intentional misinterpretation of the results to say that Republicans “make up” vaccine injuries, what does this study tell us. Again, it is an ecological study and has all the limitations of such studies. On the other hand, it is consistent with a lot of what we know about the sociology of vaccine hesitancy in the age of COVID-19, namely that the demonization of the vaccines coming from the right does influence belief in those sharing political philosophy, with lower vaccination rates, for example, and more resistance to vaccine mandates. It is therefore not unreasonable to hypothesize that political orientation might affect perceptions of the cause of AEs that might be due to COVID-19 vaccination, and this study appears to confirm that hypothesis, with people in red states being more likely to report AEs associated with COVID-19 vaccines but not associated with flu vaccines. Further research will either support or contradict the finding of this study. That’s how science works. As of now, though, the study finds pretty much what, knowing what we knew before, we would have predicted it to find.
Dr. Prasad knows his audience though, having been thoroughly captured by it. That’s why he echoes their exact complaints about “misperception” and then adds these juicy bits of red meat:
The story is framed as Republicans are more likely to imagine injuries, but the truth is Dems might be more likely to brush them under the rug due to misplaced loyalty to our lord and savior St. Anthony of Fauci. Dems might suppress real injuries.
Our “lord and savior St. Anthony of Fauci”? Give me a break. If anyone wonders why I haven’t taken Dr. Prasad seriously for a very long time, the quote above should tell you why. He knows his audience and now completely caters to it. Whether he himself believes his antivax pandering anymore, only he can say, but for all practical purposes whether he believes it or not is irrelevant. His messaging is antivax even to the point where he credulously bought into one of RFK Jr.’s favorite old antivax tropes, undermined the childhood vaccination schedule. with EBM methodolatry, and echoed old antivax “do not comply” messaging, and that, unfortunately, is more than enough.