
{kind=link}
The number of developments worrisome for the future of public health in this country have been coming so fast and furious that I can’t keep up with them on a weekly posting schedule here at SBM. I had hoped to write about something other than COVID-19 and vaccines, but unfortunately, there’s been another development in the past few days. That’s after last week, when I noted that former President and Republican nominee for President Donald Trump had cozied up to Robert F. Kennedy, Jr., who’s been a rabid antivax loon for nearly two decades now (at least), leading them both to come up with a riff on Trump’s “make America great again” (MAGA) slogan, namely “make America healthy again” (MAHA). Let’s just say that it wasn’t the greatest slogan—MAHA?—and RFK Jr.’s plan was a mixture of the not-bad (e.g., concern about regulatory capture) with the absolute bonkers (e.g., giving half of the NIH budget to research into “holistic” therapies) and, tellingly and conveniently enough, mentioned absolutely nothing about vaccines. It’s as if RFK Jr. and Trump both thought that we would totally forget about RFK Jr.’s two decades of antivax fear mongering and conspiracy theories. Now, hot on the heals of that disturbing news, it’s difficult for me not to take notice of the recently issued Updated Guidance for COVID-19 Boosters for the Fall and Winter 2024–2025 Season from the Florida Department of Health, currently run by COVID-19 contrarian and now arguably antivax physician Dr. Joseph Ladapo, discouraging the use of mRNA-based COVID-19 vaccines for older people (and that’s not all) based on misrepresented science and antivax tropes.This guidance was sent by email last Thursday to all licensed healthcare providers in the state of Florida.
Before I discuss just how off-base this “guidance” is and what it says about the danger to public health in this country, I can’t help but note that Dr. Jonathan Howard just posted a good summary of what I’m talking about when I point to the fact that RFK Jr. has been appointed honorary co-chair of Trump’s transition team, should Trump win in November. What, exactly, “honorary co-chair” means or entails is unclear, but what is clear is that RFK Jr. has managed to achieve considerable influence in the Trump campaign and will likely himself score a major cabinet position, the most likely position being Secretary of Health and Human Services, a truly horrifying prospect given that he would then have control over the Centers for Medicare & Medicaid Services (CMS), the FDA, the CDC, and the NIH are parts of HHS. Of course, for this to happen, Republicans would also have to retake control of the Senate, given that the chances that a Senate controlled by Democrats would ever confirm someone like RFK Jr. for HHS, speculation has thus already begun as to who, if Trump wins, might score leadership positions in these government agencies critical to medicine and public health. Jonathan and I have speculated that contrarian physicians like Drs. Vinay Prasad, Scott Atlas, Jay Bhattacharya, and, yes, Joseph Ladapo might be up to head the FDA, CDC, and the like. (I think it less likely that someone bonkers will be appointed to the NIH, but that could just be wishful thinking if Trump retakes power and RFK Jr. becomes HHS secretary.)
This brings us back to Dr. Ladapo. If you want to see the direction that the federal government will likely take if Trump becomes President again and RFK Jr. oversees the appointment of federal officials overseeing public health agencies, such as the FDA Commissioner and CDC Director, look no further than Florida, where COVID-19 contrarianism, hostility to public health, and outright antivax misinformation have taken over the Department of Health of a large state.
“Updated guidance”? More like the same old misinformation
So let’s look at what the updated guidance regarding COVID-19 boosters for the winter season says. I note that, almost certainly (for reasons that I will discuss shortly) Dr. Ladapo had a great deal of influence in these guidelines. They begin with a dog whistle to antivaxxers:
The Florida Department of Health (Department) is reminding health care providers of the importance of remaining up to date with current literature related to COVID-19 vaccines and boosters, and the importance of providing patients with informed consent.
Remember, whenever you see someone hostile to vaccines invoke “informed consent,” what they virtually always really mean is something that, over the years I’ve referred to as “misinformed consent” or, more recently, “misinformed refusal.” What do I mean by those terms? I mean that, under the seemingly unobjectionable cloak of a bedrock principle of medical ethics, informed consent, what is really being fed to you is at best a biased—and at worst utterly incorrect or made-up—summary of the evidence designed to portray vaccines in the worst possible light and falsely imply that the risks outweigh the benefits. Trying to produce misinformed refusal in an audience is, of course, a tactic not limited to antivaxxers. Quacks use it too, to frighten you away from conventional medicine.
Now comes the spin designed to provoke misinformed refusal, first the semi-reasonable but painted in the worst possible light:
On August 22, 2024, the United States Food and Drug Administration (FDA) approved and authorized updated versions of mRNA vaccines from Pfizer-BioNtech and Moderna. The FDA approved the vaccine for people 12 and older and provided emergency use authorization for children 6 months to 11 years old. The stated target of these boosters is the Omicron variant which is not causing a significant number of infections.
The most recent booster approval was granted in the absence of booster-specific clinical trial data performed in humans. Furthermore, this booster does not protect against the currently dominant strain, accounting for approximately 37% of infections in the United States. There are currently limited data to inform whether these boosters offer any substantial protection against the virus and subsequent circulating variants. Although randomized clinical trials are normally used to approve therapeutics, the federal government has not required COVID-19 vaccine manufacturers to demonstrate their boosters prevent hospitalizations or death from COVID-19 illness.
Notice the methodolatry, defined as the profane worship of the double-blind randomized clinical trial (RCT) above all other forms of evidence and devoid of context regarding whether an RCT would be feasible or practical. Basically, when you see someone invoking RCTs regarding updated vaccines to target variants, you are very likely looking at methodolatry that weaponizes EBM against public health and vaccines to sow doubt and mistrust. The implication is that large RCTs need to be done when updating a vaccine to target the predominant strains of a virus in circulation, when in fact the practice adopted for COVID-19 vaccines is similar to what we have long done with influenza vaccines.
It is, of course, true that if the experts picking the strains to include in the yearly update to the seasonal influenza vaccine pick wrong, which has occasionally happened in the past, the efficacy of the vaccine will be disappointingly low, compared to years when they prognosticate accurately regarding the strains expected to circulate that season. One can argue how accurately scientists have chosen the strain of SARS-CoV-2 to include in this year’s update to the vaccine, but Dr. Ladapo’s argument goes beyond that to imply that the strains chosen have resulted in an ineffective vaccine. Moreover, one might even question whether everyone needs a yearly COVID-19 booster, as Dr. Paul Offit did last year, but that’s not what Dr. Ladapo is doing here either. Worse, as you will see, in contrast to what Dr. Offit was arguing, namely that boosters should be targeted to those at highest risk for severe disease and death from COVID-19, what Dr. Ladapo appears to be doing is discouraging the use of mRNA vaccines in that very population, in addition to young people who, as antivaxxers have long deceptively argued, are at such low risk that vaccines are unnecessary.
That’s why I contrast the spin that Dr. Ladapo’s department places on the situation, which is to imply that a mismatch means that the vaccine won’t work, to a more sober assessment from a less “contrarian” scientist, Andy Pekosz, PhD, a professor in Molecular Microbiology and Immunology, who contributed to an article published by the Johns Hopkins Bloomberg School of Public Health, What to Know About the Updated COVID Vaccine for Fall, Winter 2024–25:
As in previous years, there are mRNA vaccines—one from Moderna, one from Pfizer—and a protein-based vaccine, from Novavax. One nuance this year is that the mRNA and protein-based vaccines target different—though closely related—variants.
The updated mRNA COVID vaccines from Moderna and Pfizer are based on the KP.2 strain, one of the FLiRT variants that have been spreading since early spring. These variants and their sub-variants have caused the majority of infections during this summer’s COVID wave. The protein-based Novavax vaccine is based on the JN.1 variant, which accounted for the majority of COVID infections in the first few months of 2024 and is the parent strain from which KP.2 and other currently circulating variants branch from.
At the end of the day, laboratory experiments show that all of the updated vaccines available this season can recognize circulating COVID variants and therefore should be similarly effective in reducing your chance of becoming severely ill from COVID infection or needing to be hospitalized.
As you can see, Dr. Ladapo is trying to persuade you that the new vaccines are likely to be ineffective because they supposedly target the “wrong” strains of SARS-CoV-2 compared to the strains that are currently circulating, when in fact the strains are very similar, meaning that vaccinating against one will likely provide adequate protection against the other related strains. Indeed, that is exactly the rationale cited by FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) in making its recommendations to manufacturers:
The committee unanimously voted to recommend a monovalent JN.1-lineage vaccine composition. Following the vote, the committee discussed considerations for the selection of a specific JN.1 lineage SARS-CoV-2 strain (e.g., JN.1 or KP.2) and expressed a strong preference for JN.1.
During this meeting, the advisory committee was informed of the manufacturing timelines, and they reviewed the available data. These data included information on the circulation of SARS-CoV-2 virus variants, current vaccine effectiveness, human immunogenicity data of current vaccines against recently circulating virus variants, the antigenic characterization of circulating virus variants, animal immunogenicity data on new candidate vaccines expressing or containing updated spike components, and preliminary human immunogenicity data on JN.1 candidate vaccines.
Based on the totality of the evidence, on June 6, 2024, FDA initially advised the manufacturers of the licensed and authorized COVID-19 vaccines that the COVID-19 vaccines (2024-2025 Formula) for use in the United States beginning in fall 2024 should be monovalent JN.1 vaccines.
FDA has continued to monitor the circulating strains of SARS-CoV-2. Based on the most current available data, along with the recent rise in cases of COVID-19 in areas of the country, the agency has further determined that the preferred JN.1-lineage for the COVID-19 vaccines (2024-2025 Formula) is the KP.2 strain, if feasible. This change is intended to ensure that the COVID-19 vaccines (2024-2025 Formula) more closely match circulating SARS-CoV-2 strains. FDA has communicated this change to the manufacturers of the licensed and authorized COVID-19 vaccines. The agency does not anticipate that a change to KP.2 will delay the availability of the vaccines for the United States.
I can see here from this why Moderna and Pfizer based their vaccines on the KP.2 strain and Novavax stuck with the JN.1. It’s simple logistics. Because the vaccines by Moderna and Pfizer are mRNA-based, it’s way easier for them to change the sequence of the template used to make the mRNA to be included in the vaccine and quickly ramp up manufacturing than it is for Novavax, whose vaccine uses recombinant protein as the antigen, which takes longer to make because there are the additional steps of making and purifying the protein product to be packaged in the vaccine.
Let’s look at the final “guidance” here, and then in the next section I’ll point out the antivax tropes used to come up with the “guidance”:
Based on the high rate of global immunity and currently available data, the State Surgeon General advises against the use of mRNA COVID-19 vaccines. Any provider concerned about the health risks associated with COVID-19 for patients over the age of 65 or with underlying health conditions should prioritize patient access to non-mRNA COVID-19 vaccines and treatment.
You read that right. Dr. Ladapo is advising against the use of any mRNA vaccines, period. I kid you not. He’s advising against them for everybody and only grudgingly saying that they might be used in older people and those with underlying chronic health conditions, you know, those who have been known since the beginning of the pandemic to be among the populations at the highest risk for severe disease and death from COVID-19, but only after prioritizing “patient access to non-mRNA COVID-19 vaccines and treatment.” WTF? Seriously, all treatments for COVID-19 are “non-mRNA,” because only the Moderna and Pfizer vaccines are mRNA-based, not any treatments for COVID-19 that I’m aware of. One wonders if he’s implying that doctors should encourage the use of ineffective treatments like ivermectin, but I could be reading too much into it. Maybe.
Now let’s look at the rationale cited. You will recognize several common antivax tropes. Indeed, Dr. Ladapo made it very clear that he’s conspiracy mongering in his post on X, the hellsite formerly known as Twitter, in which he accuses public health authorities of “gaslighting” the public regarding vaccines and dons the mantle of being all about The Real Science:
“Acknowledge serious safety concerns”? You mean the minor or nonexistent safety concerns that antivaxxers have been flogging for nearly four years? and the “many people who believe they’ve been injured by these vaccines”? You mean like the ones who have been fooled into thinking that their cancers—excuse me, “turbo cancers”—were caused by the vaccine?
Seriously, even though this “guidance” seems semi-reasonable if that’s all you read, Dr. Ladapo can’t help but give the game away when he’s on social media. Also note how he says at the end, “See my latest guidance.” Not “see the Florida Department of Health’s latest guidance,” but “see my latest guidance.” You can see why I refer to this document as being all Dr. Ladapo and refer to it as his. I’m just taking my lead from the crank himself.
How not to justify “updated guidance”
Right before the “guidance” in bold, Dr. Ladapo suggests that “they” are either hiding evidence or at least not providing sufficient evidence to assuage the fears of the public (fears that, I note, have been stoked by antivaxxers) over “serious safety concerns”:
Additionally, the federal government has failed to provide sufficient data to support the safety and efficacy of COVID-19 boosters, or acknowledge previously demonstrated safety concerns associated with COVID-19 vaccines and boosters, including:
- prolonged circulation of mRNA and spike protein in some vaccine recipients,
- increased risk of lower respiratory tract infections, and
- increased risk of autoimmune disease after vaccination.
Later in the “guidance,” Dr. Ladapo claims as a risk:
Elevated levels of mRNA and spike protein from the mRNA COVID-19 vaccine persist among some individuals for an indefinite period, which may carry health risks.
I’ve discussed concern number one above, the “prolonged circulation of mRNA and spike proteins” in “some” vaccine recipients. I note that the word “some” is doing a lot of heavy lifting there. For example, the half-life of the mRNA for spike protein used in the Pfizer and Moderna vaccines is on the order of a few days, with the spike protein being detectable for at most eight weeks in “some” patients. While it is true that one study oft-cited by antivaxxers found vaccine mRNA fragments in the blood as long as 28 days after vaccination, I note that this was mostly mRNA fragments, meaning that the mRNA would not be expected to generate further spike protein. Indeed, the authors speculated that this finding might have been due to slow leakage of the lipid nanoparticles out of the injection site. In any event, contrary to what antivaxxers claim, neither the modified mRNA nor the spike protein coded for by that mRNA persist long term in the human body, and there’s no evidence that their observed persistence is unsafe.
As for the last two? Regarding the claimed increased risk of lower respiratory tract infections associated with COVID-19 vaccination, I note that no studies were cited, unlike the other concerns later in the document. I do remember studies showing an increase in other infectious diseases associated with the lifting of COVID-19 restrictions after the vaccines became available, such as this one from Israel. However, you know what increases your risk of subsequent lower respiratory infections? That’s right, COVID-19 does, and the risk increases with each reinfection. As for the last one, there is no robust evidence linking COVID-19 vaccination to any autoimmune diseases, later in the “guidance” Dr. Ladapo claims:
The mRNA COVID-19 vaccine may be associated with an increased risk of autoimmune diseases including systemic lupus erythematosus (SLE), rheumatoid arthritis, and psoriasis.
But what did that study actually conclude? Not exactly what Dr. Ladapo tried so much to imply above:
We report that the risk of developing most AI-CTDs did not increase following mRNA vaccination, except for systemic lupus erythematosus with a 1.16-fold risk in vaccinated individuals relative to controls. Comparable results were reported in the stratified analyses for age, sex, mRNA vaccine type, and prior history of non-mRNA vaccination. However, a booster vaccination was associated with an increased risk of some AI-CTDs including alopecia areata, psoriasis, and rheumatoid arthritis. Overall, we conclude that mRNA-based vaccinations are not associated with an increased risk of most AI-CTDs, although further research is needed regarding its potential association with certain conditions.
See what I mean?
Many among the rest of the “risks” come straight out of the fever swamp of COVID-19 antivax nonsense. I’ll start with some of the most egregious before moving to the just exaggerated, starting with—you guessed it!—”turbo cancer” and the claims that the mRNA vaccines “permanently alter your DNA”:
Potential DNA integration from the mRNA COVID-19 vaccines poses unique and elevated risk to human health and to the integrity of the human genome, including the risk that DNA integrated into sperm or egg gametes could be passed onto offspring of mRNA COVID-19 vaccine recipients.
Oh, no! The vaccines are going to corrupt our DNA! Actually, no they are not, and the study cited by Dr. Ladapo above was an infamous one by Kevin McKernan, who has done his best to torture science to demonstrate that somehow, against all of what we know about molecular biology and what it takes for DNA to integrate into the genome, that nasty and supposedly “massive” DNA contamination from the vaccine is affecting your DNA. It’s not, and I discussed that very study in gory detail a long time ago. It’s utter nonsense. That Dr. Ladapo would cite such ideologically motivated horribly bad “science” to support his “guidance” should tell you all you might want to know.
But let’s look at some more claims:
- “The mRNA COVID-19 vaccines present a risk of subclinical and clinical myocarditis and other cardiovascular conditions among otherwise healthy individuals.”
- “The mRNA COVID-19 vaccine may be associated with an increased risk of postural orthostatic tachycardia syndrome (POTS).”
Here’s the interesting thing. As anyone who’s paid attention to the real issue of an elevated risk of myocarditis after vaccination with the mRNA vaccines knows, that risk occurs primarily in young people, in particularly young men, who nearly all make a full recovery, not the over-65 population who are most at risk of severe disease and bad outcomes if they catch COVID-19. As Dr. Paul Offit put it regarding Dr. Ladapo’s attempt to frighten everyone, including older people, away from the mRNA-based vaccines:
“It’s just such a dangerous game he plays,” said Offit, who has served on the FDA’s independent vaccine advisory committee. “You only have a roughly 1,000 times greater likelihood of dying [from Covid] if you’re over 65 than if you’re under 18.”
“The mRNA vaccines are remarkably safe,” he added.
As for POTS, yes, there is a small increased risk of POTS after vaccination, but the risk of POTS is much higher after COVID-19; specifically a recent study in Nature Cardiovascular Research concluded that COVID-19 infection is associated with a five-fold greater risk of POTS than COVID-19 vaccination. I can’t help but notice how Dr. Ladapo cited this exact study but failed to mention this or that the odds ratio for post-vaccination POTS was 1.10, quite low. Funny that. Actually, no, it’s not funny. It’s predictable given that Dr. Ladapo is an antivax crank.
I also can’t resist letting Dr. Peter Hotez also chime in:
In other words, Dr. Ladapo is either lying by admission or just plain lying, although one does have to allow for the possibility that he’s a true believer and his ideology has blinded him to what the totality of evidence shows.
Finally, there’s this:
Throughout the pandemic, studies across geographic regions found that the mRNA COVID-19 vaccines are associated with negative effectiveness after four to six months. As efficacy waned, studies showed that COVID-19 vaccinated individuals developed an increased risk for infection.
I can’t help but note that the first study cited concluded:
Effectiveness against COVID-19 hospitalization and death was 70–80% after the second dose and >90% after the booster dose. mRNA-1273 vaccine protection showed similar patterns. mRNA vaccines provide comparable, moderate, and short-lived protection against symptomatic BA.1 and BA.2 Omicron infections, but strong and durable protection against COVID-19 hospitalization and death.
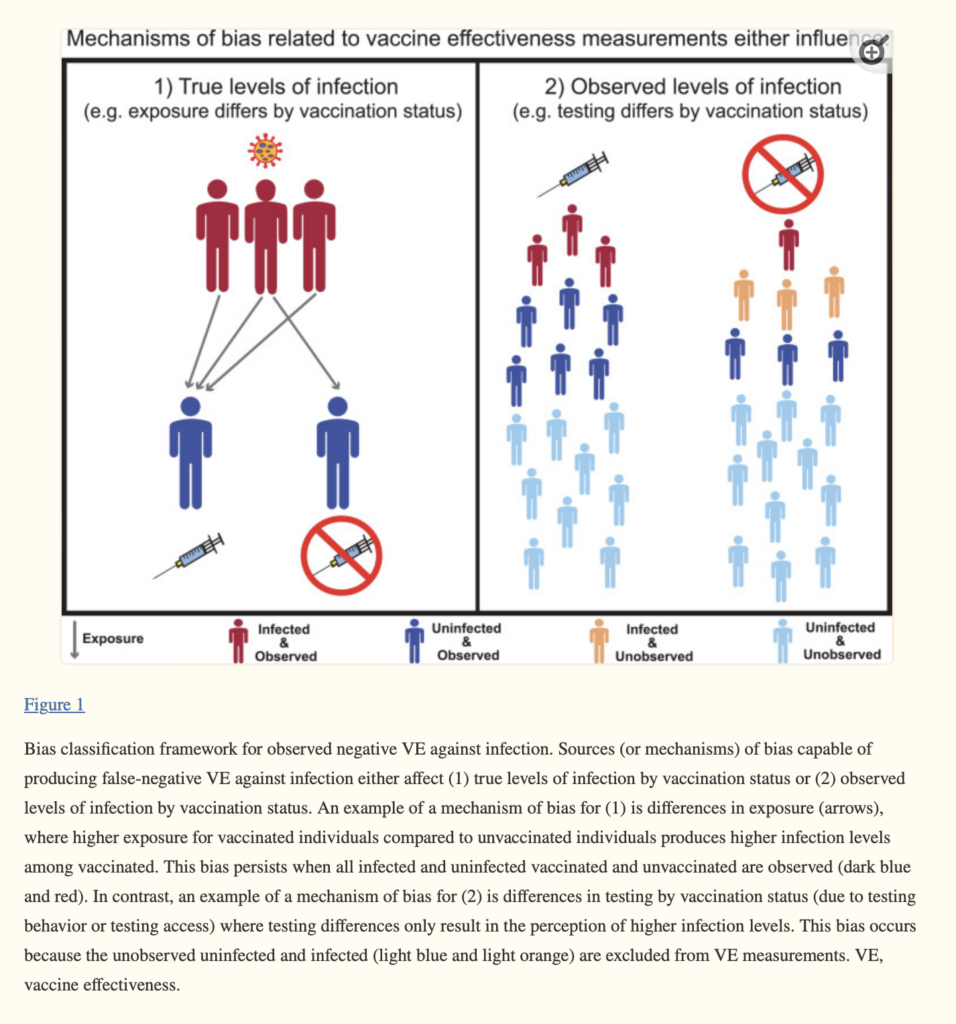
Moreover, the findings of “negative vaccine efficacy” are likely an artifact of biases related to measuring the true versus observed levels of infection in some observational studies in which exposure and testing of individuals vary based on vaccination status, as this commentary describes:
Different sources of bias produce negative VE by influencing either (1) the true levels of infection or symptomatic infection by vaccination status (e.g., by differences in exposure) or (2) the observed levels of infection or symptomatic infection by vaccination status (e.g., by differences in testing) (Figure 1). Although the biases related to (1) cause true underlying (symptomatic) infection differences that exist even given perfect sampling, biases related to (2) cause a perception of differences that do not reflect the real (symptomatic) infection levels present in the population. Although both categories of bias are important to discuss in the broader context of VE studies, their relevance for a specific study will depend on the type of VE being measured. The biases related to (1) and (2) can both influence VE measurements of infection and symptomatic infection; the biases related to (2) are less likely to play a role when measuring VE against severe outcomes (e.g., intensive care unit admission, intubation, and death) because testing for these outcomes is unlikely to differ across vaccinated and unvaccinated individuals [14].
I recommend reading the whole commentary, as it points out how these biases can give a false appearance of “negative efficacy,” and this figure is worth looking at too, as it summarizes the issues:
One notices that antivaxxers always cherry pick these studies and ignore the overall totality of the evidence, which shows that COVID-19 vaccines are safe and effective and reduce your chance of severe disease that can result in death. It’s no surprise that Dr. Ladapo does the same thing. Nor is it any surprise that he implies that the following will help as much or more than the vaccines:
Improving habits and overall health help manage and reduce the risk of heart disease, type 2 diabetes, and obesity, risk factors for serious illness from COVID-19.
The State Surgeon General and the Department continue to encourage Floridians to prioritize their overall health by:
- Staying physically active,
- Minimizing processed foods,
- Prioritizing vegetables and healthy fats, and
- Spending time outdoors to support necessary vitamin D levels.
This is the same sort of false dilemma that antivaxxers have long used. Sure, you’ll be healthier if you stay physically active and prioritize healthy eating, although staying outside is a two-edged sword if you don’t also avoid excessive sun exposure that can increase your risk of skin cancer. As for all of this supposedly reducing your risk of COVID-19, this is a trope that COVID-19 contrarians were spewing before there was even a vaccine, when, for instance, Dr. Aseem Malhotra attacked Krispy Kreme for providing free doughnuts to frontline healthcare workers in the UK and claimed that “metabolic optimization” could cure COVID-19. Everything old is new again. Too bad most people, including many of my colleagues, don’t recognize that.
Florida public health pseudoscience: Coming soon to the federal government?
When Florida Governor Ron DeSantis first appointed Dr. Ladapo as Florida’s Surgeon-General and therefore the person in charge of the Florida Department of Health and the state’s entire public health apparatus, many of us were justifiably alarmed, an alarm that has been totally validated by his performance since his appointment. After all, Dr. Ladapo was a founding member of America’s Frontline Doctors, which made a name for itself in that horrible first summer of the pandemic by touting hydroxychloroquine as a miracle cure for COVID-19 and later turned to telehealth grift selling prescriptions for ivermectin to cure COVID-19, and a signatory of the Great Barrington Declaration, the document published by contrarian scientists brought together by a right-wing think tank to advocate a social Darwinist “let ‘er rip” approach to the pandemic with poorly defined “focused protection” for those most at risk for severe disease and death from the pandemic.
Moreover, this “updated guidance” is far from the first time that Dr. Ladapo has tried to mislead using the usual denialist techniques of cherry picking evidence and even outright misrepresenting it. Last year, he was busted for altering a Florida Department of Health study for lying with statistics to make it look as though the vaccine was more dangerous than COVID-19 for men under 40. Earlier this year, consistent with its inclusion in this “guidance,” Dr. Ladapo was parroting McKernan’s bad science that massively exaggerated the problem of DNA contamination of the vaccine.
Given the recent developments in which Donald Trump has cozied up to RFK Jr. and (apparently) promised him a cabinet-level position in his administration, should he win in November, it’s very easy to foresee what will happen to medicine, public health, and science in general if Trump becomes President again. You need look no further than Florida, except that it could even be worse than Florida. After all, Dr. Ladapo isn’t the only doctor hostile to vaccines and public health science who would likely find a leadership position in a second Trump administration. There is ample reason to be afraid, very afraid.