{kind=link}
Over the last week or two, you might have noticed a disturbance in the alternative medicine force. Unlike disturbances in the Force in Star Wars movies (which usually result from horrors like the obliteration of millions of lives on Alderaan), this was a joyous disturbance in the mystical nonexistent energy fields in which promoters of alternative medicine cancer cures and haters of chemotherapy and “conventional” cancer treatment (the two almost always go together) thought that a major study in a reputable journal had put yet another “final nail in the coffin” of chemotherapy. Or at least they could spin the study as an indication that chemotherapy is nothing more than an expensive toxic brew foisted on an unsuspecting public by the nefarious shadowy forces of Big Pharma in order to extract maximal resources from third party payers, which, to them, is almost as good. Of course, they do this with any study that suggests chemotherapy isn’t as effective as people would like, but this study seemed on the surface like powerful ammunition. It’s not. It’s an interesting preclinical study showing a mechanism by which chemotherapy given before surgery (neoadjuvant chemotherapy) might promote the spread of some cancers. Whether the findings are clinically important remains to be seen.
“Alternative cancer cure” advocates and salesmen rejoice
Although it’s an interesting study with somewhat of a cautionary note, it’s far less of a “black eye” to chemotherapy (as Jeffrey Jaxen put it over at that repository of science misinterpreted to promote alternative or “natural” medicine, Sayer Ji‘s GreenMedInfo), than advertised. Meanwhile, Chris Wark of “Chris Beat Cancer” (hint: surgery, not the quackery he pursued, took care of his colon cancer) practically exults that “chemo may spread breast cancer and trigger more aggressive tumors.” Of course, the real gloating comes from—who else?—Mike Adams, who proclaims the study a “Medical BOMBSHELL” showing that chemotherapy has been found to spread cancer. He also can’t help but throw in the lies he’s been peddling about me:
The cancer industry is a corrupt, criminally-operated branch of modern medicine, run by felony criminals and hucksters like Dr. Farid Fata who is currently serving prison time for falsely diagnosing people with cancer so he could profit from chemotherapy treatments they didn’t need. His colleague, Dr. David Gorski of the Karmanos Cancer Center in Detroit, is not yet in prison but has been reported to the FBI for investigation. He remains one of the sickest and most sociopathic abusers of women in the history of cancer surgery, earning him the nickname “Gorski the Nipple Ripper.” He has also been accused of promoting cancer-causing medical interventions, possibly as a means to further his own profit interests at the expense of the health of innocent women. Dr. David Gorski has also been linked to “skeptics” kingpin James Randi, who was caught on tape soliciting sex acts from a young male.
Yawn. I guess I can expect another paragraph like this inserted into pretty much any rant against chemotherapy that Adams writes. It’s my badge of honor, I guess. Oh, well. Word to Mikey: I used to be upset by your smear campaign against me—about a year ago. These days, however, I’m laughing at you, not with you, because your lies are so transparently over the top that no one but your hardcore followers would even have a chance of believing them. I was never a “colleague” of Dr. Fata, who never worked at my cancer center, and that “nipple ripper” name came from Patrick “Tim” Bolen, a man who used to be cancer quack Hulda Clark’s most vigorous defender. I also note that it was Adams himself who claimed to have reported me to the FBI (something conveniently not mentioned). That was well over a year ago. Neither I nor anyone I know has been contacted by the FBI or my state attorney general (where Adams also claims to have filed a complaint). I suspect his “criminal complaints,” if they were ever filed at all, ended up in the “crank file,” where they belong.
Sorry for that diversion. It seemed…necessary. Let’s get back to what less insane-sounding (but equally mistaken) alternative cancer cure advocates are saying, after which then I’ll delve into the study itself and show you why, although it is a reason for some concern, it’s not evidence that chemotherapy doesn’t work, and, in fact, if validated by further studies, points the way to overcoming what might be a significant problem in cancer chemotherapy. In discussing this study, Jaxen, for instance, lists all the usual suspects of studies trotted out by the anti-chemotherapy brigade every time they feel a rant coming on. For example, he invokes what I like to call the “2% gambit,” citing, as all who use this gambit do, a single Australian study from around 16 years ago that left out a lot of chemotherapy-sensitive tumors and willfully confused adjuvant chemotherapy with chemotherapy delivered as primary treatment for curative intent. Basically, he sees the study as “more evidence” of this:
By now, many are beginning to understand that one of the problems with chemotherapy is that it doesn’t address the underlying cause(s) of cancer. Chemotherapy originated from an idea and consciousness that was far from idealistic. The whole generation of chemotherapeutic drugs that are being used today, and there are over one hundred of them, developed from poisonous nerve gas created for warfare. As reported in 2012 by Green Med Info, cancer is the second leading cause of death in the developed world, and yet much of the medical and research communities are still in the dark ages when it comes to treating and understanding it. However, in the age of information, great strides are being made by doctors and researchers who are going against the grain of the failed convention ‘wisdom’ in cancer treatment. In addition, individuals are beginning to take responsibility by educating themselves.
Of course, for all their claims of “addressing the underlying cause” of cancer, alternative medicine cancer cure mavens always fail to show how their favored nostrums do any better on that score, much less that they are actually more effective than conventional treatments—or even that they’re effective at all.
Chris Wark chimes in with the same propaganda:
As I’ve said many times, chemotherapy is often only a short-term solution to a long-term problem.
The new study presents evidence that chemotherapy can switch on a repair mechanism in the body which ultimately allows tumours to grow back stronger. It also increases the number of ‘doorways’ on blood vessels which allow cancer to spread throughout the body.
At least Wark admits that chemotherapy can sometimes be at least a “short term solution” to cancer. Again, nothing Wark discusses shows how his preferred methods do anything to “address the underlying cause” of the long term problem of cancer. We know that diet and certain environmental exposures can modulate cancer risk for certain cancers, but once the cancer is already established it’s too late for that.
So now that we’ve seen ideology in action, let’s look at science in action.
How chemotherapy is used to treat cancer
Before I get to the study, in order to help readers not familiar with how chemotherapy is used to treat cancer, I feel obligated to provide a brief primer. There are four main ways that chemotherapy is used to treat cancer:
Curative: Chemotherapy can be the primary (and sometimes only) treatment for cancer. This is common in hematological malignancies, like leukemia and lymphomas, where it’s usually some combination of chemotherapy ± radiation therapy that is curative. Surgery is rarely indicated. The intent here is to use chemotherapy to eliminate cancer from the body.
Adjuvant chemotherapy: After definitive surgical treatment of the primary cancer, chemotherapy is administered to decrease the chance of recurrence. This is a very common use of chemotherapy, particularly in breast cancer and colorectal cancer. Indeed, the use of adjuvant chemotherapy for breast cancer since the 1980s, among other factors, has contributed to a decline in breast cancer mortality of around 30% since 1990.
Neoadjuvant chemotherapy: Neoadjuvant chemotherapy is administered before surgery. In general, there are two main reasons to administer neoadjuvant chemotherapy: (1) to shrink a tumor to make a non-operable tumor (e.g., one stuck to major structures) operable for cure; and (2) to make organ-sparing surgery possible. This latter use is common in breast cancer in order to shrink a tumor so that a mastectomy is not required to remove it and breast-conserving surgery is possible. Moreover, in breast cancer, it is known from numerous studies that neoadjuvant chemotherapy results in equivalent results as adjuvant chemotherapy. Overall survival and disease-free survival and time to locoreginal recurrence are the same, whether chemotherapy is administered before or after surgery. The same idea is used in the surgical treatment of low rectal cancer requiring an abdominoperineal resection (APR) to remove. An APR involves removing the anal sphincter and leaving the patient with a permanent colostomy. With neoadjuvant chemotherapy, it is often possible to shrink the tumor enough to make sphincter-sparing surgery possible, something very desirable to patients, the vast majority of whom understandably recoil at the idea of requiring a permanent colostomy.
Palliative chemotherapy: In stage IV disease, chemotherapy is often used to palliate symptoms from growing tumors and can prolong life, although not result in long term survival. This is also a common use of chemotherapy.
The study that the likes of Mike Adams and Chris Wark are crowing over examines neoadjuvant chemotherapy. That’s an important point. It does not apply to other uses of chemotherapy. Think of it this way. Adjuvant chemotherapy is quite different from neoadjuvant chemotherapy in one way. The primary tumor is not present when adjuvant chemotherapy is administered. All that’s left are microscopic tumor deposits that could turn into metastases. Those are what adjuvant chemotherapy targets, because chemotherapy is much better at wiping out microscopic tumor deposits than macroscopic tumors. Contrast that to neoadjuvant chemotherapy, which targets both those same microscopic tumor deposits and also targets the main tumor, which is usually large. (Remember the reasons why neoadjuvant chemotherapy is administered.)
Comparatively speaking, there are many orders of magnitude more cancer cells in the neoadjuvant setting than in the adjuvant setting. If spread of tumor due to neoadjuvant chemotherapy were a major factor clinically, we’d expect survival using neoadjuvant chemotherapy before surgery to be worse than using it after surgery. That we don’t see that is a good reason to be at least a little skeptical of how clinically relevant the results of this study will turn out to be. Indeed, I’ve never ceased to be amazed that, in breast cancer and most cancers for which neoadjuvant chemotherapy is used, the survival benefit provided by chemotherapy (adjusted for tumor stage and other relevant characteristics, of course) is the same regardless of whether the chemotherapy is administered before or after surgery. Even better, neoadjuvant chemotherapy can give an indication of how “nasty” (i.e., resistant to chemotherapy) a tumor is, based on how much (or how little) it shrinks in response to chemotherapy. Moreover, pathologic complete response (that is, a response so dramatic that the tumor not only disappears clinically but the pathologist can’t find any viable tumor cells in the resected specimen) is an excellent prognostic factor predicting favorable outcomes.
Keep these things in mind as I discuss the study.
Does neoadjuvant chemotherapy “spread” cancer?
So let’s take a look at the study itself (Karagiannis et al, “Neoadjuvant chemotherapy induces breast cancer metastasis through a TMEM-mediated mechanism“), which was published in a Science journal, Science Translational Medicine by a group at the Albert Einstein College of Medicine. Reading the abstract, I quickly realized—surprise! surprise!—that the findings were considerably more nuanced and interesting than Adams, Wark, and Jaxen presented. I also quickly realized that the purpose of the study was to identify potential problems with how neoadjuvant works in order to find strategies to make it work better. Of course, doing research to make existing therapies better is complex, and the authors noted that increasing tumor cell dissemination could “diminish the clinical benefit” of neoadjuvant chemotherapy. Note the distinction. It is known—sorry, couldn’t resist a Game of Thrones reference given that as I write this the season seven premiere is only a few hours away—from numerous studies that neoadjuvant chemotherapy produces a survival advantage for breast cancer patients in addition to the advantages it produces in making inoperable tumors operable or making it possible for women who would otherwise lose their breast to preserve it. Tumor cell dissemination as a result of chemotherapy reduces, not eliminates, that benefit, and it certainly does not “make cancer spread” in such a way that neoadjuvant chemotherapy is worse than no chemotherapy. Yet that’s what the cancer quacks strongly imply.
So what is the mechanism being examined here? Previous work has demonstrated one mechanism by which breast cancer cells can gain access to blood vessels and spread. In this mechanism, breast cancer tumor cell spread occurs at microscopic structures dubbed tumor microenvironment of metastasis (TMEM). Each TMEM is composed of three cell types, all in direct physical contact with each other: a tumor cell making a protein that regulates a structural protein (actin) known as Mammalian-enabled (MENA), a perivascular macrophage (an immune cell near the blood vessel), and an endothelial cell (the cell type that lines blood vessels). Vascular permeability due to TMEM has been shown to be localized and mediated by vascular endothelial growth factor–A (VEGF-A) release from the TMEM-bound macrophages, which express the angiopoietin receptor TIE2. Now, I used to do a lot of work with VEGF-A back in the 1990s, when I studied tumor angiogenesis, the process by which tumors interact with their environment to stimulate the ingrowth of new blood vessels. Basically, the macrophages associated with TMEM secrete this factor, which increases vascular permeability, making “holes” through which tumor cells can gain entry to the blood vessel and spread via blood. However, only tumor cells expressing high levels of MENA can take advantage of this. (Note that there are different isoforms—variants—of Mena that are pro-invasion and anti-invasion; when we refer to MENA here, we’re mostly referring to the MENAINV.) Tumors with a high TMEM “score” in animal models have a higher likelihood of metastasis compared to tumors with low TMEM scores.
The authors hypothesized that preoperative chemotherapy could increase the density and activity of TMEM sites in breast cancer, as well as an increase in invasion-promoting MENA isoforms, and thereby increase the number of tumor cells spreading. They based their hypothesis on the observation that one chemotherapy agent, paclitaxel (a.k.a. Taxol), induces an influx of macrophages into the primary tumor and that macrophages are required for TMEM assembly. The hypothesis was tested using a transgenic mammary tumor model in which mouse mammary tumor virus–polyoma middle T antigen was introduced to produce a mouse strain that spontaneously develops mammary tumors at a high rate, patient-derived xenografts (PDXs, which are tumors derived from patients that can grow in mice with defective immune systems), and pre- and post-neoadjuvant breast cancer tissue samples from human patients. There are also all sorts of pretty images from intravital imaging (IVI, which allows imaging of living animals at a cellular level) that a researcher needs if he wants to publish in a journal like Cell, Science, or Science Translational Medicine. I don’t mean that so much as a knock on the authors given that the paper is actually good, but rather as a sarcastic aside at what it takes these days to be published in top-tier journals. Besides, several of the authors have an extensive background in imaging research; so I can’t really fault them for using it. It is, after all, so much cooler to look at these complexes in living mice than to do what they had to do in humans and test fixed tissue from biopsies and surgical specimens.
The authors addressed their hypothesis using multiple tumor models, including the MMTV-PyMT mice, another mouse strain bearing tumors transplanted from the MMTV-PyMT mice, and two PDX models, (HT17 and HT33, for anyone who’s interested). Animals were treated with various chemotherapeutics and compared to controls, with the tumors imaged, levels of various RNAs and proteins compared, and tumors assessed. Key findings were as follows:
- Paclitaxel at the dose used delayed tumor growth (as expected) but increased TMEM assembly by as much as three-fold.
- Paclitaxel increased the infiltration of perivascular macrophages in the primary breast cancer microenvironment.
- Paclitaxel induced TMEM-dependent vascular permeability in breast tumors.
- Paclitaxel increased metastatic dissemination of breast tumors (roughly a two-fold difference, although the result wasn’t statistically significant for one tumor model—Figure 3I). This was confirmed by examining the lungs of the mice, where investigators found an increase in both microscopic metastases in the paclitaxel-treated mice and single-cell metastases (two-fold increase).
- Paclitaxel promotes the expression of invasive isoforms of Mena in breast tumors, and dissemination required Mena.
- Levels of circulating tumor cells in the bloodstream increased in response to chemotherapy.
- Treating mice with doxorubicin and cyclophosphamide (two other drugs commonly used in standard-of-care breast cancer treatment) produced similar changes in the primary tumors and their surrounding microenvironment.
Finally, when the investigators tested human breast cancer tissue before and after neoadjuvant chemotherapy with paclitaxel followed by combined doxorubicin/cyclophosphamide, they found this:
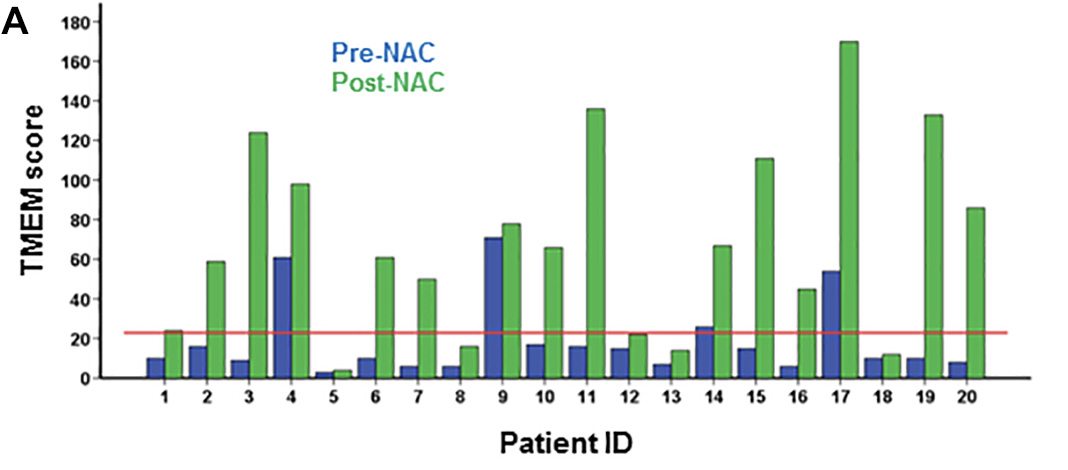
Areas staining positive for MENA also increased. Pretty striking, I’ll agree. However, remember what I said above. Neoadjuvant chemotherapy is still quite effective.
More importantly, consider this final result. In the same mouse models, blocking the TIE2 receptor with rebastinib decreased the number of perivascular macrophages and blocked the increase in circulating tumor cells to the level of controls without affecting TMEM assembly. This means that TIE2 inhibition blocks the function of TMEM sites but not their assembly. Fortunately, in these mouse models, that was enough. More importantly, it also suggests a strategy for making neoadjuvant chemotherapy work better in patients, as illustrated here:
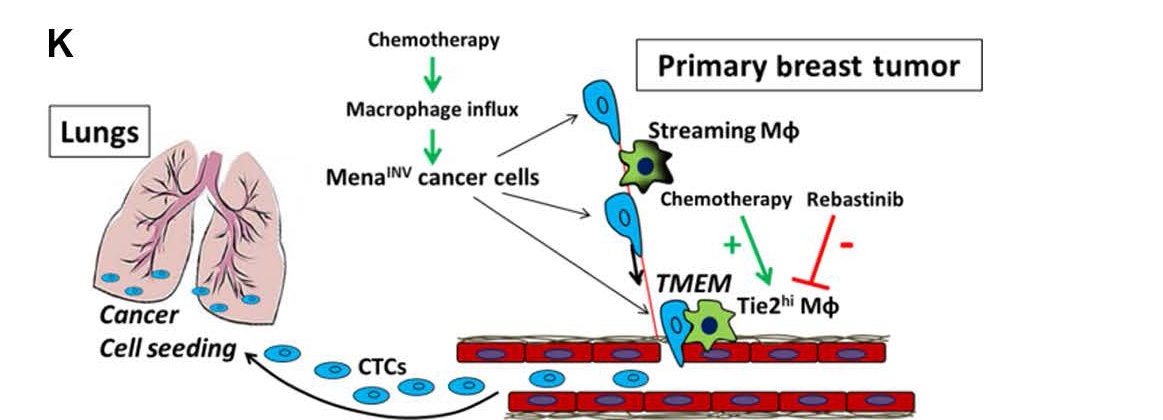
Note that there are multiple points that can be attacked to overcome the stimulation of more invasiveness by chemotherapy.
Putting it all together
If there’s one thing that distinguishes science-based medicine (SBM) from the sort of medicine advocated by those promoting alternative cancer cures, it’s that SBM is always trying to make things better. When it is observed that, for instance, neoadjuvant chemotherapy might not be having as strong an effect on tumors as it could, scientists look for the reason why. If that reason why happens to be that some forms of chemotherapy might increase the ability of cells from the primary tumor to spread, decreasing the benefit of neoadjuvant chemotherapy, they look for the molecular and cellular mechanisms responsible for that problem and then try to find ways to exploit those mechanisms to overcome the problem. That’s exactly what Karagiannis et al did. So when quack-loving entrepreneurs like Mike Adams, Chris Wark, and Jeffrey Jaxen tell you this study “proves” that chemotherapy does more harm than good, they’re either ignorant or intentionally misrepresenting the results, because the study doesn’t show that at all.
It’s not just the quacks, though. Articles in mainstream news sources reported this study with headlines like “Chemotherapy could cause cancer to SPREAD and grow back even more aggressive, new study claims.” OK, that’s The Daily Mail, which is to science as The Weekly World News is to, well, news. But other stories had headlines like “Chemotherapy could spread cancer cells and lead to more advanced tumours, says study” and “Chemotherapy before breast cancer surgery might fuel metastasis.” Far better is a headline like “Neoadjuvant Chemotherapy Treatment May Increase Risk Of Breast Cancer Spreading In Some Patients“, which more accurately assesses the results of the study. In fairness, I know that editors, not reporters, determine headlines and most of the mainstream articles I mentioned did point out some of the caveats that I discussed, but the impression most people take away comes from the headline, and that impression was only marginally less scary than the headlines coming from Sayer Ji’s and Mike Adams’ websites.
More importantly, if you’re a woman considering neoadjuvant chemotherapy to treat breast cancer, don’t let the spin on this study frighten you out of it. The benefits of neoadjuvant chemotherapy include not only improved survival but the possibility of breast conserving surgery, and, as I mentioned before, there is no detectable difference in overall survival whether chemotherapy is administered before or after surgery.
As for the future, research like this could lead the way to better neoadjuvant chemotherapy. For example, a woman undergoing neoadjuvant chemotherapy might some day have biopsies done part way through the chemotherapy. If her tumor’s TMEM score has increased markedly, then I could envision the addition of a TIE2 inhibitor or other inhibitor of TMEM function being added to her chemotherapy to block the increased level of circulating tumor cells and reverse whatever increased risk of metastasis that might be attributable to neoadjuvant chemotherapy in order to produce better outcomes. That’s how SBM improves, in contrast to alternative medicine, in which no therapies are abandoned when demonstrated to be ineffective and/or dangerous and no therapies are ever improved upon.