{kind=link}
Here at Science-Based Medicine, we have been writing about the “integrative medicine” specialty known as “functional medicine” for nearly 12 years. The reason is that so-called “functional medicine” is a form of pseudomedicine that dresses itself up as scientific but at its core is deeply unscientific. Basically, its practitioners don the mantle of “science” by ordering reams of diagnostic tests that are not science-based and whose interpretation is not at all clear, all in order to “treat the cause” of disease. True, functional medicine does also include some very banal, science-based advice (weight loss, healthy diets, exercise, sufficient sleep, and the like), but in addition to “integrating” massive overtesting and overtreatment it also “integrates” quackery like homeopathy, naturopathy, traditional Chinese medicine, and chiropractic into the mix, thus diluting the science-based part to the point where it becomes difficult for the non-skeptic to tell what is and isn’t science-based. Functional medicine is also such a vague and amorphous entity that it led Wally Sampson to ask early in the history of this blog just what functional medicine is anyway and to conclude that it’s an “indecipherable babble and descriptive word salad“. As I like to say, functional medicine combines the worst features of conventional medicine (overtesting and overtreatment) with a heaping helping of quackery. Or, to apply Harriet Hall’s famous adage about naturopathy to functional medicine, what is good about functional medicine (emphasis on diet, exercise, and lifestyle) is not unique, and what is unique about functional medicine (the overtesting and quackery) is not good.
Dr. Sampson also noted, as we continue to do, that claiming to treat the “underlying cause” of a condition raises the usual straw man argument that modern medicine does not, which of course is untrue, while also implying that there are “underlying causes” known to functional medicine practitioners and not to regular physicians. Functional medicine also claims to treat chronic diseases that are (according to its advocates) inadequately treated by conventional medicine, thanks to a more “advanced” approach, both in conceptual thinking and in practical management. Of course, when you look critically at what functional medicine actually does in practice, these claims are easily shown to be nonsense. (For an example, just check out a case report that I discussed a three years ago of functional medicine used in treating an elderly woman with a nasty breast cancer.) Unfortunately, thanks to the embrace of functional medicine by the Cleveland Clinic, which in 2014 hired functional medicine guru Dr. Mark Hyman to set up a clinic there, the promotion by practitioners of “integrative medicine,” and stealth advertising in the form of news stories, functional medicine has become somewhat respectable, even though it doesn’t deserve that respect and the American Academy of Family Physicians has pointed out that it includes harmful and dangerous treatments. (Functional medicine includes a lot of diagnoses of “heavy metal toxicity” and often includes “detox” treatments to alleviate that fantasy-based diagnosis.)
It was only a matter of time before the Cleveland Clinic started publishing studies to promote functional medicine, and last week I saw this one popping up on social media as “evidence” that functional medicine does better than conventional medicine treating chronic illnesses. But does it? Let’s find out if the study matches the advertising claims the Cleveland Clinic posts on social media:
In the past 5 years, 12,122 patients from 48 states and 33 countries have come to Cleveland Clinic's Center for Functional Medicine for care. pic.twitter.com/aIf6acQLtm
— ClevelandClinicNews (@CleClinicNews) September 30, 2019
The Cleveland Clinic publishes a study advertisement for functional medicine
So late last week, I started seeing Tweets like this, either retweeted or in the various alternative medicine feeds that I follow (for blogging material):
In the first study of the functional medicine model, researchers find its associated with improvements in health-related quality of life. https://t.co/UMsq2NuG45
— ClevelandClinicNews (@CleClinicNews) October 25, 2019
Functional Medicine ! Our first Manuscript from the Center for Functional Medicine# Cleveland Clinic #health care# Functional Medicine https://t.co/gAW57fpFwI
— Dr Elizabeth Bradley (@EPBradleyMD) October 25, 2019
However, I think that the market for Functional Medicine Ventures is investing in transformational components that work with our current healthcare system while also being critical pieces to help support, enable, and accelerate the commercial viability and promise of the
— bendubin (@bendubin) October 25, 2019
So let’s take a look first at the Cleveland Clinic’s press release about the study, and then we can dive into the study itself, which you can read because it’s published in JAMA Network Open.
The Cleveland Clinic pressroom exults:
In the first retrospective cohort study of the functional medicine model, Cleveland Clinic researchers found that functional medicine was associated with improvements in health-related quality of life. The study was published today in the Journal of the American Medical Association Network Open.
The two-year study examined 1,595 patients treated in Cleveland Clinic’s Center for Functional Medicine and 5,657 patients seen in primary care at a family health center, assessing health-related quality of life using PROMIS®, an NIH-validated questionnaire. PROMIS provides a measure of patients’ global physical and mental health that can be monitored over time, measuring factors like fatigue, physical function, pain, gastrointestinal issues and emotional well-being.
The study investigated the association between the functional medicine model of care and health-related quality of life by comparing functional medicine patients with patients seen in a primary care setting.
Researchers found that patients seen by the Center for Functional Medicine showed beneficial and sustainable improvements in their PROMIS global physical health.
So, before even delving into the methods section of the study, I can see a lot of issues. The study is retrospective, for one thing, and not randomized. That means that the patients who come to Cleveland Clinic Center for Functional Medicine are likely a very different patient population from the patients who go to the Clinic’s regular primary care clinics. A lot of the tests and interventions used in functional medicine, not being evidence-based, are not covered by health insurance, which means that the patient has to pay out of pocket and, therefore, it’s very likely that the patient population seen at a functional medicine clinic will be more affluent and suburban than patients seen at a regular primary care practice run by the Clinic. In fairness, the authors do address this issue in the paper, but the question is whether they addressed it well enough. Also, spoilers: Some of the differences in populations were not what I would have expected.
Before delving into the paper itself, I feel obligated to briefly recap just what functional medicine actually is.
Functional medicine: WTF is it?
The basic “principles” of functional medicine tend to be mundane and difficult to disagree with; rather, it’s the interpretation of these principles that is problematic and embraces quackery, bad science, and pseudoscience. I’ve seen multiple versions of these “core principles” of functional medicine over the years, but they usually boil down to something like this list:
- Acknowledging the biochemical individuality of each human being, based on concepts of genetic and environmental uniqueness
- Incorporating a patient-centered rather than a disease-centered approach to treatment
- Seeking a dynamic balance among the internal and external factors in a patient’s body, mind, and spirit
- Addressing the web-like interconnections of internal physiological factors
- Identifying health as a positive vitality—not merely the absence of disease—and emphasizing those factors that encourage a vigorous physiology
- Promoting organ resilience as a means of enhancing the health span, not just the life span, of each patient
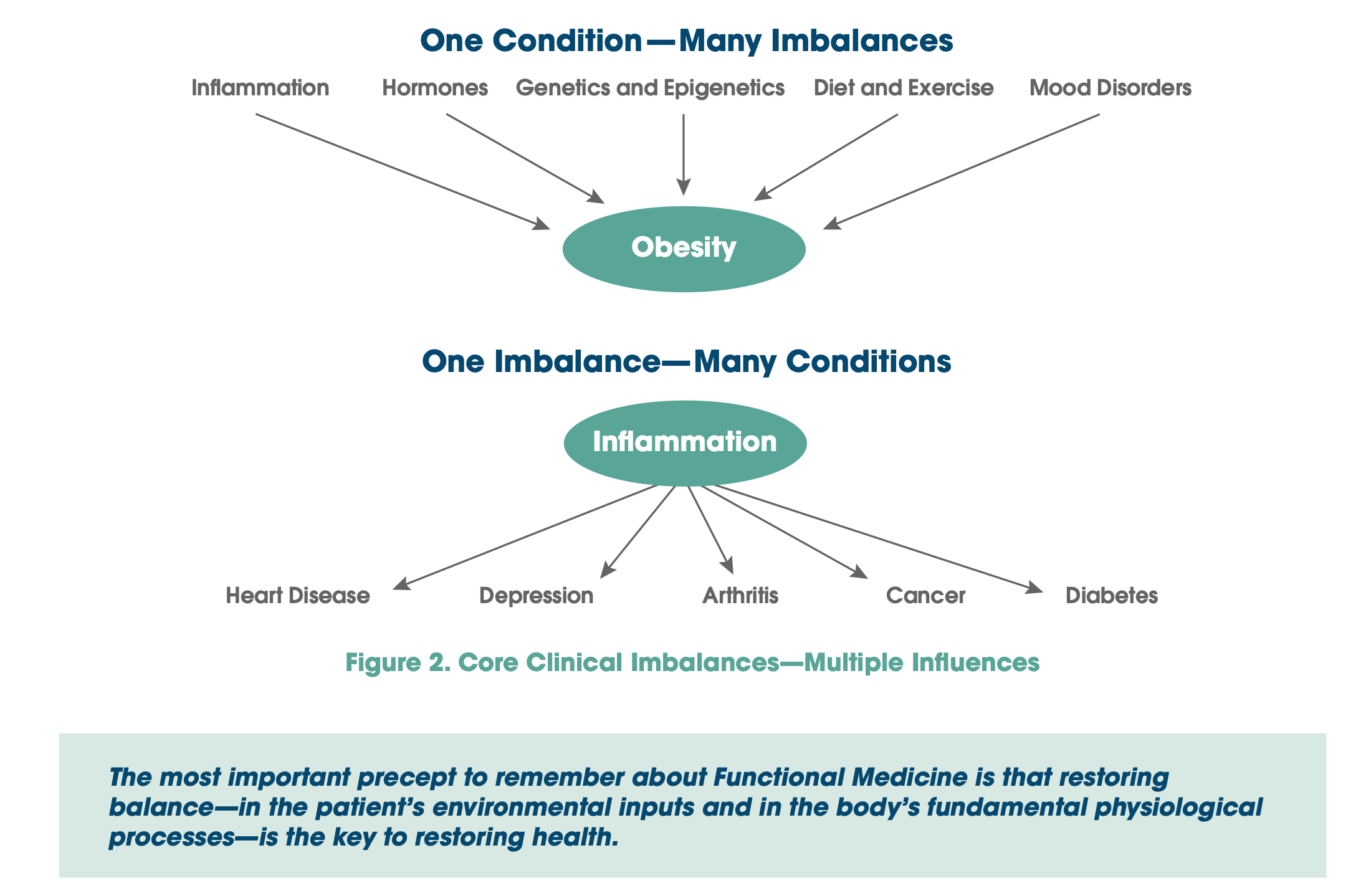
Much like traditional Chinese medicine and its invocation of “imbalances” in the five elements as a cause of disease or, for that matter, ancient European medicine and its “imbalances in the four humors,” functional medicine is all about “correcting imbalances,” only just far more “science-y” sounding than the imbalances of the aforementioned ancient forms of prescientific medicine. Specifically these imbalances:
To assist clinicians in understanding and applying Functional Medicine, IFM has created a highly innovative way of representing the patient’s signs, symptoms, and common pathways of disease. Adapting, organizing, and integrating into the Functional Medicine Matrix the seven biological systems in which core clinical imbalances are found actually creates an intellectual bridge between the rich basic science literature concerning physiological mechanisms of disease and the clinical studies, clinical diagnoses, and clinical experience acquired during medical training. These core clinical imbalances serve to marry the mechanisms of disease with the manifestations and diagnoses of disease.
- Assimilation: digestion, absorption, microbiota/GI, respiration
- Defense and repair: immune, inflammation, infection/microbiota
- Energy: energy regulation, mitochondrial function
- Biotransformation and elimination: toxicity, detoxification
- Transport: cardiovascular and lymphatic systems
- Communication: endocrine, neurotransmitters, immune messengers
- Structural integrity: subcellular membranes to musculoskeletal integrity
This set of imbalances and the principles above frequently lead to charts like this, which look profound on the surface but are really quite banal:
And this one:

The strategy functional medicine claims to use to treat patients sounds very scientific, but in reality are a lot of hot air:
- Gene-Environment Interaction: Functional Medicine is based on understanding the metabolic processes of each individual at the cellular level. By knowing how each person’s genes and environment interact to create their unique biochemical phenotype, it is possible to design targeted interventions that correct the specific issues that lead to destructive processes such as inflammation and oxidation, which are at the root of many diseases.
- Upstream Signal Modulation: Functional Medicine interventions seek to influence biochemical pathways “upstream” and prevent the overproduction of damaging end products, rather than blocking the effects of those end products. For example, instead of using drugs that block the last step in the production of inflammatory mediators (NSAIDs, etc.), Functional Medicine treatments seek to prevent the upregulation of those mediators in the first place.
- Multimodal Treatment Plans: The Functional Medicine approach uses a broad range of interventions to achieve optimal health including diet, nutrition, exercise and movement; stress management; sleep and rest, phytonutrient, nutritional and pharmaceutical supplementation; and various other restorative and reparative therapies. These interventions are all tailored to address the antecedents, triggers, and mediators of disease or dysfunction in each individual patient.
- Understanding the Patient in Context: Functional Medicine uses a structured process to uncover the significant life events of each patient’s history to gain a better understanding of who they are as an individual. IFM tools (the “Timeline” and the “Matrix” model) are integral to this process for the role they play in organizing clinical data and mediating clinical insights. This approach to the clinical encounter ensures that the patient is heard, engenders the therapeutic relationship, expands therapeutic options, and improves the collaboration between patient and clinician.
- Systems Biology-Based Approach: Functional Medicine uses systems biology to understand and identify how core imbalances in specific biological systems can manifest in other parts of the body. Rather than an organ systems-based approach, Functional Medicine addresses core physiological processes that cross anatomical boundaries including: assimilation of nutrients, cellular defense and repair, structural integrity, cellular communication and transport mechanisms, energy production, and biotransformation. The “Functional Medicine Matrix” is the clinician’s key tool for understanding these network effects and provides the basis for the design of effective multimodal treatment strategies.
- Patient-Centered and Directed: Functional Medicine practitioners work with the patient to find the most appropriate and acceptable treatment plan to correct, balance, and optimize the fundamental underlying issues in the realms of mind, body, and spirit. Beginning with a detailed and personalized history, the patient is welcomed into the process of exploring their story and the potential causes of their health issues. Patients and providers work together to determine the diagnostic process, set achievable health goals, and design an appropriate therapeutic approach.
Of course, there is nothing in the principles above that conventional science-based medicine doesn’t advocate or do. The main difference is that SBM demands adequate evidence and, for the most part, doesn’t embrace quackery. For instance, the whole bit about “gene-environment” interaction serves as an excuse for functional medicine to make all sorts of fake diagnoses, such as heavy metal toxicity (requiring “detox” such as chelation therapy, naturally), chronic Lyme disease, and chronic candida infections. Meanwhile, the emphasis on “biochemical individuality” and systems biology (which functional medicine practitioners frequently mangle beyond recognition) serves as an excuse for functional medicine practitioners to make stuff up as they go along and prescribe all sorts of supplements to “correct” supposed “deficiencies” in micronutrients, after having ordered dozens (or even hundreds) of unnecessary lab tests to find such “deficiencies.” Indeed, as a physician, I find it rather offensive that functional medicine mavens claim that conventional medicine doesn’t consider the patient in context or physiology that transcends simple organ systems. I went to medical school 30 years ago, and was taught those things then. I was also taught that you shouldn’t make stuff up or use treatments that don’t have good evidence supporting them.
On to the Cleveland Clinic’s functional medicine study
Not surprisingly for a study that’s more propaganda than science, the introduction includes this gem of functional medicine propaganda:
The functional medicine model of care provides an operating system that works to reverse illness, promote health, and optimize function by addressing underlying causes, symptoms, and functional imbalances in interconnected biological networks.10 These imbalances may impair principal biological functions (assimilation, defense and repair, energy production, biotransformation, communication, transport, and structural integrity) that result from gene-environment interactions, including lifestyle, environmental toxins, and the microbiome. Functional medicine removes triggers for illness and provides inputs to restore and optimize health. Functional medicine also addresses social determinants, including the psychological, emotional, and spiritual aspects of health and disease.11 A foundation of functional medicine is the use of food as medicine to prevent, treat, and reverse chronic disease. The functional medicine model of care may have the ability to improve patient’s health-related quality of life (HRQoL), including physical function and well-being. Therefore, the purpose of the present study was to investigate the association between the functional medicine model of care and HRQoL by comparing functional medicine with care received in a family medicine setting.
I really hate when a medical model of care is likened to a computer operating system. It’s so trite. Be that as it may, though, all the functional medicine tropes are right there in the introduction to the study, for all to see.
The study itself is a fairly straightforward retrospective cohort study, which means that the investigators looked at existing data in the Cleveland Clinic database to compare a cohort of patients seen in its functional medicine clinic with a cohort of patients seen in its primary care clinics for various outcomes, in this case, changes in the cohorts’ Patient-Reported Outcome Measurement Information System (PROMIS) Global Physical Health (GPH) scores at 6 and 12 months after their first visit. The PROMIS Global Health scale consists of ten questions that measure physical, mental, and social health, and it provides a measure of overall health:
Higher scores indicate a better health-related quality of life. PROMIS GH comprises 10 items and produces 2 summary scores: Global Physical Health (GPH) and Global Mental Health (GMH). The GPH measure includes 4 items on physical health, physical functioning, pain intensity, and fatigue, whereas, the GMH comprises 4 items on overall quality of life, mental health, satisfaction with social activities, and emotional problems. PROMIS physical function measures are sensitive enough to detect longitudinal changes due to targeted clinical interventions and able to distinguish among diverse chronic diseases.17,18 Summary scores are centered on the 2000 US Census with respect to age, sex, educational level, and race/ethnicity and are transformed to a T-score with a mean (SD) of 50 (10).14 Changes of 5 points suggest a meaningful or clinically important change; higher scores indicate a better HRQoL [health-related quality of life].
The overall study encompassed 7,252 patients (1,595 from the functional medicine center and 5,657 from the family medicine center), of which 4,780 (65.9%) were women. The mean age was 54.1 years. Corrections were made for socioeconomic status, race, etc. Interestingly, income was simply estimated by the median income reported in the 2010 census for the ZIP code where each patient resided. After propensity score matching, there were 398 patients in each group.
The results were…underwhelming, the very definition of a statistically significant but almost certainly clinically insignificant change. Just check out the chart below, remembering that a change of less than 5 points in these particular scales is not a meaningful difference.
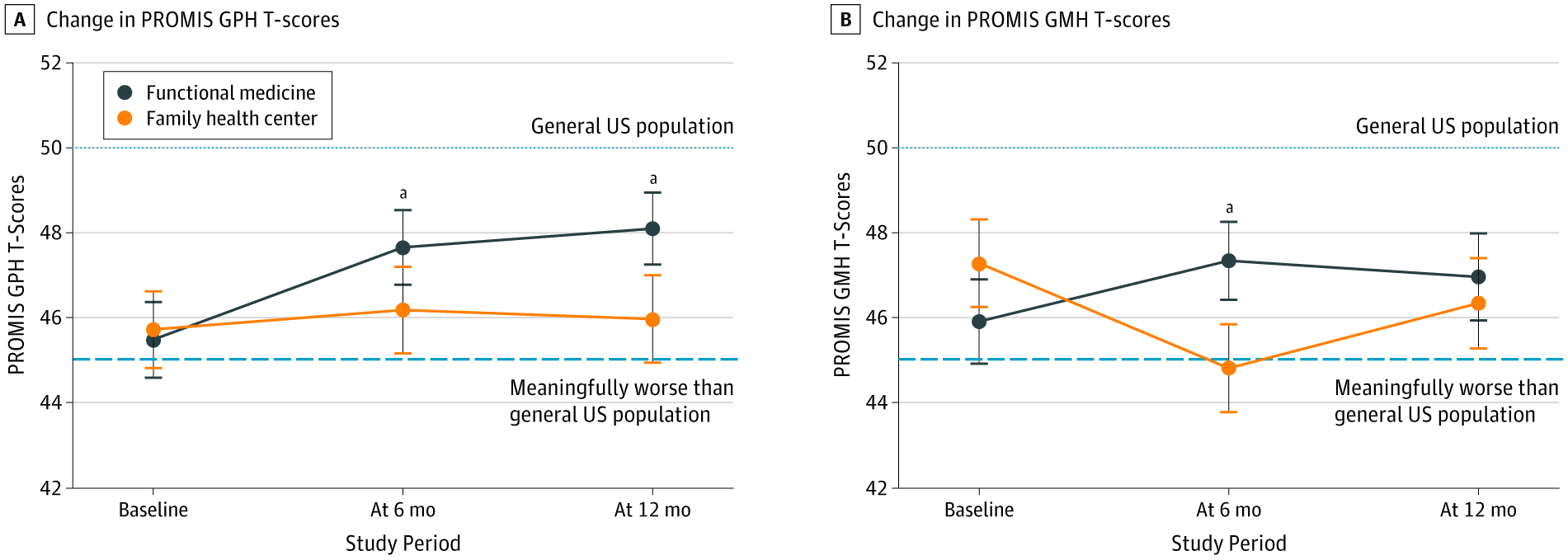
Basically, at 6 months, the functional medicine cohort had an improvement in their PROMIS GPH scores from 46.18 at baseline to 47.77 (P < .001). The PROMIS GPH mean (SD) change at 6 months was also significantly greater than that seen in patients treated at the family medicine group. At 12 months, functional medicine patients showed improvement in PROMIS GPH similar to that observed at 6 months; however, comparisons with the family medicine cohort were not significant. True, more patients seen at the Center for Functional Medicine (30.9%) improved their PROMIS GPH scores by 5 or more points than those seen at the Family Health Center (22.1%), but how meaningful is that really?.
Now look at this chart, which is particularly damning:
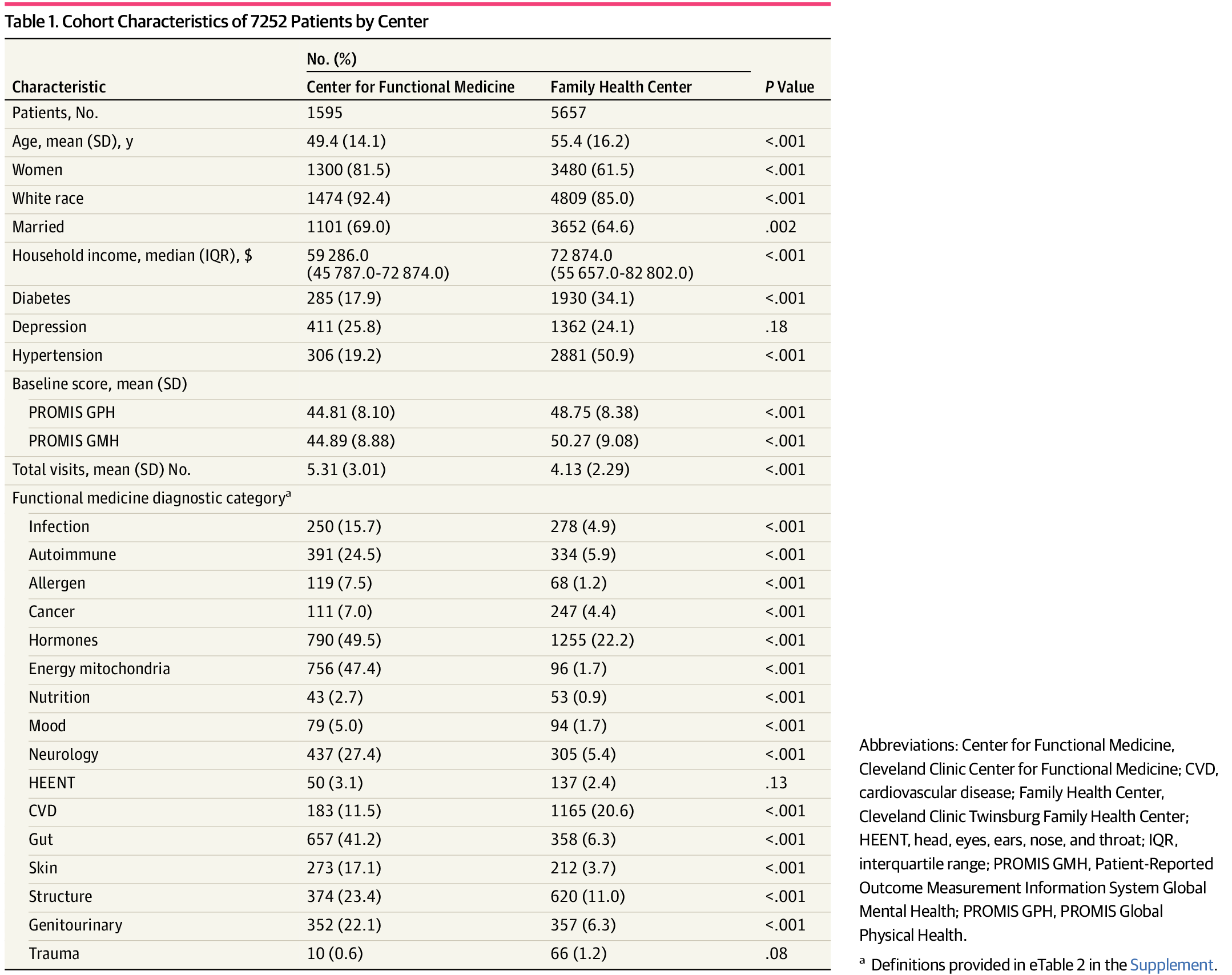
Interestingly, the median income of the functional medicine cohort was actually lower than that of the family medicine cohort, although the functional medicine cohort younger, whiter, more married, and less healthy at baseline, with a higher prevalence of hypertension and diabetes. More tellingly, the functional medicine cohort started out with a whole lot more functional medicine diagnoses, such as autoimmune diseases (functional medicine loves to diagnose nonexistent autoimmune diseases), mitochondrial disorders, “gut” issues, infections, and allergies. To me this indicates a whole lot of things being treated in the functional medicine clinic that almost certainly don’t require treatment and a whole lot of fake functional medicine diagnoses, like chronic Lyme.
I’ll give the authors some credit for acknowledging potential confounders:
Second, patients seen in the Center for Functional Medicine may be different from those seeking primary care in a family health center. Our attempt to circumvent this bias was to PS match patients from each center based on certain variables; however, there may be unmeasured confounders associated with the reported outcomes. For example, patients who request to be seen at the Center for Functional Medicine may be more motivated to make a nutrition-, lifestyle-, or behavior-related change in their life. Success with such change is associated with patient activation measures relating to engagement and self-management opportunities. Higher patient activation is also associated with individuals who perceive that they have an unmet need as it relates to their medical care. Patients seeking functional medicine may have exhausted all available opportunities in conventional medicine to manage or mitigate their chronic disease and perceive functional medicine as their only recourse. Therefore, patients seen in the functional medicine setting may be more engaged and adherent to treatment recommendations.
In which case, the answer to improve outcomes would be to figure out ways to engage patients more in their own care while using science-based medicine, not to add overtesting, overtreatment, and quackery to the mix and to justify it by saying that it motivates patients to live a healthier lifestyle. Similarly, the authors note that functional medicine doctors spend much more time with patients, with an initial consult running 60-75 minutes. Again, if that’s what it takes to help patients, then the answer isn’t functional medicine and all the quackery that it entails, but rather to find a way to pay for primary care physicians to be able to spend more time with each patient. The Cleveland Clinic requires each of its functional medicine clinic patients to consult with a registered dietitian and health coach, in addition to a clinician, as part of their initial visit. That’s not a bad idea and could potentially be adopted by conventional primary care practices (well, maybe not the health coach, as insurance probably wouldn’t pay for that), again with no association with quackery required.
None of this stops the Cleveland Clinic from saying:
“This is a first-of-its-kind study to evaluate the impact of functional medicine model of care on patients’ health-related quality of life. In the past, evidence to support the model has been primarily anecdotal, published as case reports or based on specific, targeted interventions used as part of the functional medicine approach, such as nutritional changes,” said Michelle Beidelschies, Ph.D., director of Research and Education for the Cleveland Clinic Center for Functional Medicine and the lead author of the study. “Functional medicine practitioners have suggested that their patients are improving with a systems-based approach to chronic disease. Now, they have evidence that their approach is associated with improved quality of life.”
I must emphasize that this study doesn’t show improved health outcomes due to functional medicine. Its primary outcomes were scores on subjective scales, not any measured hard outcome, such as blood pressure control, incidence of complications (i.e., strokes in patients with hypertension or blindness or loss of limbs in diabetics). Worse, it didn’t even really show what the very scales used consider to be a meaningful or significant improvement in health-related quality of life. It’s basically a whole lot of nothing, far more PR than anything else, and I expect that this study will be used to market functional medicine and try to convince conventional doctors that functional medicine has merit.