
{kind=link}
Chiropractors would like to reinvent themselves as family doctors. I’ve written about that before and Jann Bellamy has written about it here, here, here, and here. A new study in The Journal of Chiropractic Education alleges that the National University of Health Sciences is nearing its institutional goal of training chiropractic students as primary care practitioners. The data they collected don’t even begin to support that assertion. The study is not only meaningless, it demonstrates a gross misunderstanding of the education required to practice competent primary care.
Traditional education of MDs
The 4 years of medical school are very different from those of a chiropractic school. When I was a student, the first two years were spent in classrooms and labs studying gross anatomy, physiology, pharmacology, pathology, biochemistry, histology, neuroanatomy, microbiology, immunology, embryology, and other meaty science subjects. In the 3rd year, students moved into the hospital wards, rotating through internal medicine, surgery, pediatrics, OB/GYN, psychiatry, neurology, radiology, emergency medicine, etc. 4th year clinical rotations involve a higher level of responsibility and include electives. Most of the clinical experience is with seriously ill hospitalized patients, but students also get some outpatient clinic experience.
The real training begins after graduation, when students get to put their learning into practice. They assume primary responsibility for patients, under supervision. I did what was called a “Rotating 0” internship, designed to provide a broad foundation before entering a specialty. I rotated through internal medicine, surgery, OB/GYN, pediatrics, and electives (neurology and ENT). Most of my time was spent on the hospital wards, but I also worked in outpatient clinics and in the ER. The experience was intensive, with call every 3rd night. This meant working all day, all night, and the following day for a total of 32+ hours straight, followed by a day when we worked 9-10 hours and got to go home in the evening. In my case, my training was interrupted by an Air Force assignment as a General Medical Officer, and after that I spent 2 years in a 3-year residency in Family Practice (my internship counted for year 1). Residencies are where doctors get their training in a specialty, with graduated responsibilities as the program proceeds. At 3 years, the family practice residency is one of the shortest; a surgery residency typically lasts 5 years, a neurosurgery residency 7 years. In some cases, a residency is followed by a fellowship in a subspecialty, such as gastroenterology or child psychiatry. Rigorous exams are required at various stages of training and for board certification in a specialty.
Changes in recent years
Since I graduated, there have been new developments. There are limits to the number of consecutive hours a resident can work; medical schools are integrating classroom training with clinical experiences in various ways; there is a new designation of “hospitalists” who care for inpatients admitted by other doctors. Some primary care and even some specialty care is carried out by nurse clinicians and physician assistants with lesser levels of training than MDs, training more focused on what they will actually be doing in practice. PA training typically involves 2-3 years of postgraduate study, and most PA students have previous health care experience.
Chiropractic education
Chiropractic education is much less rigorous. Class time is taken up by many hours of training in manipulation technique like “toggle,” and “cervical technique,” palpation, and “subluxation” analysis; and for subjects like financial management and practice management. They don’t get any experience caring for seriously ill hospitalized patients. There is no internship or residency. The NUHS calls students in its student clinic “interns,” but that bears no resemblance to what “intern” means in medical training. The training it offers is in line with the purpose of the Council on Chiropractic Education, and they state “students at NUHS are educated and clinically trained to become primary care physicians. To become an effective primary care provider, a student intern must be prepared to identify, manage, and refer successfully when necessary a broad scope of conditions that include musculoskeletal and nonmusculoskeletal problems.”
The NHUS study
The study’s purpose was to quantify the number of musculoskeletal and nonmusculoskeletal cases NUHS interns treat during the clinic component of their education and to compare the results to data available for chiropractic and “allopathic” providers. The method was a retrospective chart review based on diagnostic codes. Of a potential 173 patients scheduled to be seen in the specified time frame (one trimester), 8 were no-shows, 27 denied consent, and 25 patients had no treated diagnoses, leaving only 113 patient files to be analyzed.
The results: 297 coded diagnoses, 76% of these musculoskeletal. Treated diagnoses: 52.2% musculoskeletal only, 12.4% nonmusculoskeletal only, and 35.4% both musculoskeletal and nonmusculoskeletal. This compared to 83% musculoskeletal and 17% nonmusculoskeletal diagnoses for practicing chiropractors, and 10% musculoskeletal and 90% nonmusculoskeletal diagnoses for “allopaths.”
Diagnoses not represented: neoplasms, blood disorders, diseases of the circulatory system, complications of pregnancy, childbirth and puerperium, and perinatal conditions. Out of 113 patients, only one was under the age of 20, and none were under the age of 11. Here is the list of diagnostic categories:
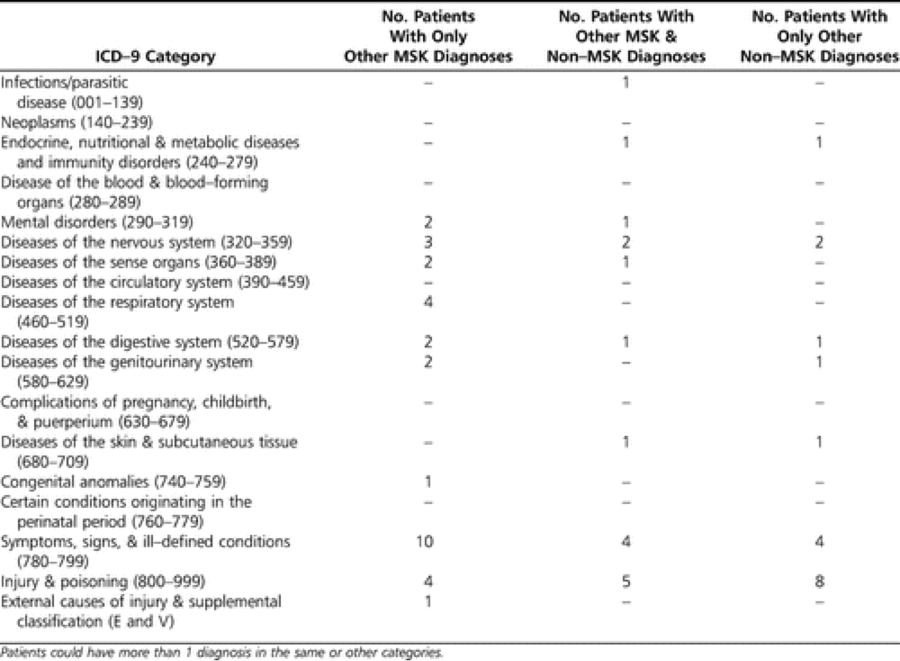
Note that the list of categories includes only 1 infection, 2 endocrine, nutritional and metabolic diseases, 4 diseases of the respiratory system, 4 diseases of the respiratory system, 3 diseases of the genitourinary system, 2 diseases of the skin, and there are several categories with no patients at all. These are just categories, they don’t tell us the actual diagnoses, whether they amounted to what has been called “snotology” (minor complaints like colds) or more serious disorders.
They don’t say how many students were involved, but elsewhere I found that 84 students are enrolled in the program. Surely no one student could have seen more than a few patients or seen a full spectrum of these diagnoses.
The authors point out another serious problem: diagnoses like hypertension or diabetes mellitus were not treated by students, but were “monitored or appropriately referred.”
Comparison to primary care
Contrast that to the 25 most common diagnoses seen in primary care: hypertension, hyperlipidemia, and diabetes lead the list, followed by back pain, anxiety, obesity, allergic rhinitis, reflux esophagitis, respiratory problems, hypothyroidism, visual refractive errors, osteoarthritis, fibromyalgia/myositis/neuritis, malaise and fatigue, joint pain, acute laryngopharyngitis, acute maxillary sinusitis, major depressive disorder, acute bronchitis, and asthma.
The chiropractic students all put together saw a total of only 2 patients who fell into one of the categories of the top 3 conditions presenting to primary care providers. As defined by the CCE, primary health care is:
Care that is provided by a health care professional in the patient’s first contact within a health care system that includes an examination and evaluation, diagnosis and health management. A Doctor of Chiropractic practicing primary health care is competent and qualified to provide independent, quality, patient-focused health care to individuals of all ages and genders by: (1) providing direct access, portal of entry care that does not require a referral from another source; (2) establishing a partnership relationship with continuity of care for each individual patient; (3) evaluating a patient and independently establishing a diagnosis or diagnoses; (4) managing the patients [sic] health care and integrating health care services including treatment, recommendations for self-care, referral and/or co-management.
Conclusion
How could anyone possibly imagine that the findings of this study show that the school is approaching the goal of “training students to become primary health care providers”? You would have to be delusional to think that. They saw no children and no patients with the top 3 conditions presenting to a primary care office. The numbers tabulated were for the entire group of students, with no indication of the numbers seen by any individual student.
It’s just plain stupid to think that simply listing diagnostic categories could establish the adequacy of training.
Apart from the inadequacies of clinic training, there is a glaring defect: chiropractors don’t have inpatient hospital experience with responsibility for the care of seriously ill patients. Without that experience, how could they be expected to develop good judgment about when to refer and when hospitalization is necessary?
Chiropractors are not qualified to provide primary care. This study only reinforces that fact.