
{kind=link}

And so 2026 begins…
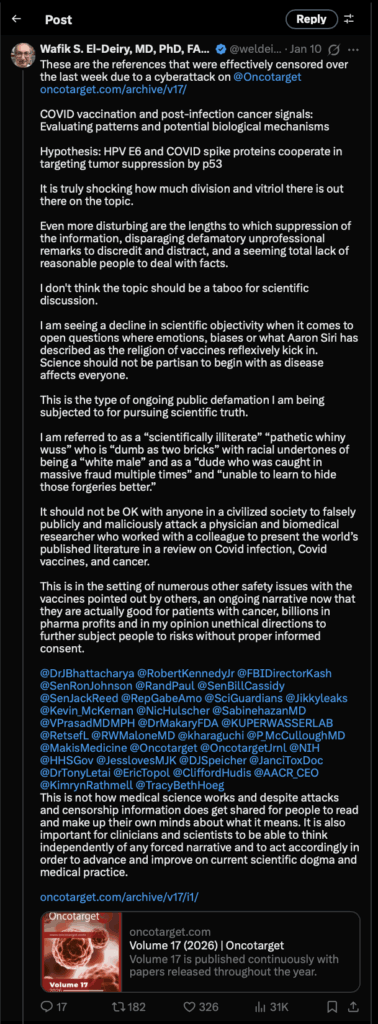
As I sat down last week to write the first post of 2026, I had been thinking that I would write about this week’s topic, but after thinking about it I decided to address a more general question of whether it is ever a good idea to debate science deniers. Then, as I sat down to write this week, there were the news stories about how the longtime antivax activist who is now Secretary of Health and Human Services, Robert F. Kennedy Jr., had unilaterally decided to remake the CDC-recommended vaccine schedule in the image of Denmark because Denmark vaccinates against the fewest diseases of any European Union country. However, that was over a week ago, and Steve had already discussed it. (That’s not to say that I might not address, either here or at my not-so-super-secret other blog, it as part of RFK Jr.’s broader war on the vaccine schedule, but I felt less impetus to do it now.) Then, over the weekend, I saw a post on X, the disinformation hellsite formerly known as Twitter, by eminent oncologist and cancer researcher Dr. Wafik El-Deiry (whom we’ve met before here) touting his review article (not really a “study”) in which he wildly speculated about links between COVID-19 vaccines and cancer. True, he didn’t call them “turbo cancers,” but he did parrot the headline calling the vaccines “jabs”:
A couple of observations. First, the review article in question, COVID vaccination and post-infection cancer signals: Evaluating patterns and potential biological mechanisms, co-authored by Charlotte Kuperwasser and Wafik S. El-Deiry, was officially published on January 3, and it was on or about that date when Dr. El-Deiry started flogging a narrative in which a cyberattack on the journal website, OncoTarget, had kept the article from being viewed. The “Daily Fail” is bad enough as a source, but then Dr. El-Deiry posted:
Yes, you read that right. He posted an Infowars link about his review article. However, that wasn’t the worst, at least not in my not-so-humble opinion:
Children’s Health Defense? Seriously? If CHD were ever to praise and publicize a study or review article that I’d authored or co-authored, I would not be proud of it. Quite the opposite. I’d be deeply ashamed, to the point where I’d STFU and reexamine my entire professional life, scientific activities, and belief systems before daring to reemerge, most likely humbled and apologetic, especially if I had made the enormous reputation-damaging mistake that Dr. El-Deiry did. I quote from the CHD article:
Wafik El-Deiry, M.D., Ph.D., one of the co-authors, told The Defender that the paper “is the first most comprehensive presentation summarizing the world‘s literature on the subject matter of COVID vaccines, COVID infection and cancer.”
He said some of the review’s findings “look like a smoking gun” linking COVID-19 shots to cancer.
Karl Jablonowski, Ph.D., senior research scientist for Children’s Health Defense, said the review’s findings may represent “the tip of a very damaging iceberg.”
“It is not remotely surprising that a gene-therapy rebranded as a vaccine, never tested for oncogenic safety, with severe immune dysregulating effects, injected into a billion people would correlate with an increased risk of cancers worldwide,” Jablonowski said.
El-Deiry said the review may provide insights into rising cancer rates in recent years, including an increase in so-called “turbo cancers.”
“I believe there is a risk of cancer associated with COVID vaccination,” El-Deiry said. “The magnitude of the risk remains to be more precisely defined, including the risk of hyperprogression.” Hyperprogression refers to cases where “a pre-existing tumor grows more aggressively.”
Seriously, Dr. El-Deiry. Giving an interview to CHD’s publication, The Defender, is not a good look for any legitimate scientist, but it’s even worse than that. Since last weekend (at least), Dr. El-Deiry has been flogging a claim that he’s being “censored” because of a cyberattack on OncoTarget, the journal that published his review article, a claim for which he has presented no evidence and that he blames on PubPeer, a website that exists to do postpublication review of scientific articles. Much of the discussion there is about the methodology, design, and quality of various scientific papers. However, what PubPeer is best known for—one might even say notorious for—is the exposure of image manipulation in the scientific papers. These criticisms and demonstrations of image manipulation can lead to corrections and sometimes even to retractions of scientific papers. One particularly controversial aspect (at least among scientists) of PubPeer is that it allows anonymous commentary and goes to great lengths to protect the anonymity of its commenters when they are threaten with libel suits.
Before I move on, I will admit that I have mixed feelings about the anonymity of PubPeer commentary. On the one hand, anonymity allows junior researchers to be safer in criticizing the work of more senior and entrenched researchers who could destroy their careers. On the other hand, anonymity can be a mask behind which malicious actors can cause mischief. That being said, as long as I’ve been following PubPeer commentary and stories on Retraction Watch, I have seen little or no evidence that anonymous commentary finding evidence of image manipulation has been malicious. Indeed, most of the examples that I’ve seen of image manipulation uncovered on PubPeer seem to be due to carelessness and lax oversight of trainees as the prepare scientific manuscripts than due to intentional fraud. Moreover, some of the most famous contributors to PubPeer are not anonymous. (Elizabeth Bik comes to mind.)
Why did I discuss PubPeer? It will become apparent shortly. First, let’s look at what OncoTarget says about the alleged cyberattack, without presenting any evidence whatsoever for these charges:
In December 2025 and January 2026, our server encountered malicious cyberattacks that led to disruptions of online publications and website access.
The Dark side of PubPeer: there are suspicions that certain individuals associated with PubPeer may have been involved in cybercriminal activities, including hacking servers, causing journal websites to go offline, and using illegitimate practices to influence Google search results for journals and scientists.
It turns out that PubPeer has nearly 100 threads about papers authored or co-authored by Dr. El-Deiry. I am not going to comment on the validity of these threads here—that would take enough effort for at least one more post, and I want to stick to my originally intended topic—other than to note that Dr. El-Deiry, like a number of researchers whose papers are unflatteringly dissected by PubPeer commenters, very much resents being called out on PubPeer. Indeed, as Leonid Schneider at For Better Science noted on Friday:
El-Deiry has been battling his PubPeer critics for some time now, mostly on X where he also directly or via proxies runs the account Science Guardians. Their favourite hate targets are Elisabeth Bik, Kevin Patrick and yours truly.
ScienceGuardians, I note, claims to do basically the same thing as PubPeer, only anonymity is not permitted, and those running the site claims to use “stringent verification” that contributors are legitimate academics, which sounds a bit elitist, even to me. Also, hilariously, if you look at a the ScienceGuardians entry for a recent excellent study showing that, contrary to the narrative being pushed by antivax “turbo cancer” cranks there isn’t a huge amount of DNA contamination, you’ll see that the commenters included antivax cranks like Jessica Rose and Kevin McKernan, with zero actual reputable legitimate academic scientists.
In any event, the post that made me finally decide to address Dr. El-Deiry’s paper was this one:
I mean, seriously. In context, Schneider was so obviously engaging in sarcasm and mockery that Dr. El-Deiry should be embarrassed to have thought it to be a real admission of guilt, particularly given the part in which Schneider claims to have been behind the vaccine-induced cancers. Also, it was pointed out on X that there probably was no cyberattack:
point out that this is an easy-to-make mistake. My not-so-super-
secret other blog once went down for a while because of the same
error. I managed to fix it without crying, “DDoS!”
With that background, I will now examine the decline of a once-great scientist through the lens of this latest incident, which demonstrates how even the best of us can fall prey to ideology-based pseudoscience. True, this is not a story on par with that of, for instance, Linus Pauling‘s descent into “vitamin C cures everything, including cancer” quackery and Luc Montagnier’s fall into alternative medicine and antivax quackery. Both were Nobel Laureates for whom I once coined the term “Nobel Disease” to describe Nobel Laureates who embraced nonsense in their later years. It is, nonetheless, very disappointing to me, as Dr. El-Deiry has made real and important contributions to oncology and the science of cancer, in particular regarding the tumor suppressor genes p21 (CDKN1A) and p53, that led me to admire his work and him quite a bit. Indeed, his work was frequently cited in my papers in the 1990s and early 2000s, and I even met him in person once many years ago. There was a period of time after I had first become aware of his tendency to jump on the antivax train to link his work with p53 to “turbo cancers” when he appeared to have quieted down and gone back to what he’s best at, tumor suppressor research, but, starting with his promotion of the misinterpreted South Korean study claiming to link COVID-19 vaccines to cancer (deconstructed by yours truly when it came out a few months ago), he seems to have re-emerged and, if anything, doubled down.
A sadly dubious review article begins
Let’s take a look at the review article on OncoTarget, COVID vaccination and post-infection cancer signals: Evaluating patterns and potential biological mechanisms, co-authored by Charlotte Kuperwasser and Wafik S. El-Deiry. The first thing I noticed was the rapid turnaround time, with the manuscript submitted November 26, accepted December 26, and published on January 3. Another thing that really struck me is the open peer review (which I’ll discuss after the article). It makes me wonder who the peer reviewers were, given that these were some of the most milquetoast “critiques” I’ve seen and many of them missed the point of the big flaws in this “study.” I wonder even more based on this footnote to the paper:
The Editor-in-Chief, Dr. Wafik S. El-Deiry, was not involved in the peer-review process or the decision-making for this paper. Dr. El-Deiry shared the submitted manuscript with National Cancer Institute (NCI) Director Anthony Letai by email electronically on December 12, 2025.
So, even if Dr. El-Deiry “was not involved in the peer-review process or the decision-making for this paper,” he is the editor-in-chief of the journal. While I applaud him somewhat for trying to take the decision-making out of his own hands, I still have to wonder whether others involved with the journal would be willing to tell him that this paper didn’t meet peer-review standards. Basically, even though Dr. Letai apparently shepherded the manuscript through the peer-review process, it is nonetheless a major conflict of interest for an editor-in-chief to submit a manuscript like this, particularly one that can be easily predicted to be controversial, to his own journal. It was bad enough when John Ioannidis was publishing dubious papers in a journal for which he had recently served as editor-in-chief, but this is worse.
Before I get into the nitty-gritty, let’s cite the abstract of this review, so that everyone knows the broad outline of what the review claims to have done and to have found:
A growing number of peer-reviewed publications have reported diverse cancer types appearing in temporal association with COVID-19 vaccination or infection. To characterize the nature and scope of these reports, a systematic literature search from January 2020 to October 2025 was conducted based on specified eligibility criteria. A total of 69 publications met inclusion criteria: 66 article-level reports describing 333 patients across 27 countries, 2 retrospective population-level investigations (Italy: ~300,000 cohort, and Korea: ~8.4 million cohort) quantified cancer incidence and mortality trends among vaccinated populations, and one longitudinal analysis of ~1.3 million US military service members spanning the pre-pandemic through post-pandemic periods. Most of the studies documented hematologic malignancies (non-Hodgkin’s lymphomas, cutaneous lymphomas, leukemias), solid tumors (breast, lung, melanoma, sarcoma, pancreatic cancer, and glioblastoma), and virus-associated cancers (Kaposi and Merkel cell carcinoma). Across reports, several recurrent themes emerged: (1) unusually rapid progression, recurrence, or reactivation of preexisting indolent or controlled disease, (2) atypical or localized histopathologic findings, including involvement of vaccine injection sites or regional lymph nodes, and (3) proposed immunologic links between acute infection or vaccination and tumor dormancy, immune escape, or microenvironmental shifts. The predominance of case-level observations and early population-level data demonstrates an early phase of potential safety-signal detection. These findings underscore the need for rigorous epidemiologic, longitudinal, clinical, histopathological, forensic, and mechanistic studies to assess whether and under what conditions COVID-19 vaccination or infection may be linked with cancer.
My first reaction was that the term “growing number of peer-reviewed publications” supposedly supporting a link between COVID-19 vaccines and cancer is doing a lot of heavy lifting here. Second, I noted that these 69 reports only encompassed 333 patients with cancer, which, when weighed against the literally billions of doses of COVID-19 vaccines administered to billions of people, is a truly infinitesimally tiny number of cancer reports. Remember what I said as the vaccines started rolling out? Whenever you administer so many doses of a product to so many billions of people, there will be cases in which adverse events occur within close temporal proximity to vaccination by random chance alone, even highly implausible adverse events. I always like to bring up the example of, for instance, a person who receives a vaccine and then the next day dies due to a piece of granite falling off of a building hitting them in a rare freak accident and coincidence. How do investigators determine that these rare cancers aren’t just a different example like the one I just mentioned? There are, of course, statistical methods to do that.
In any case, here’s a table that describes the literature surveyed:
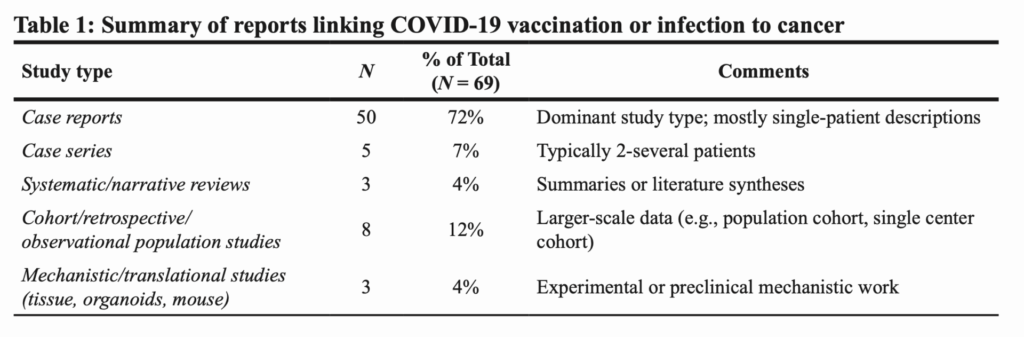
Notice how the vast majority of the papers analyzed are case reports. I’ve discussed a number of these case reports myself, and I’ve found none particularly convincing for a mechanistic link between COVID vaccines and cancer, much less “turbo cancers.” Anyone wanna bet whether I see some of those papers here? Before I get into the case reports and studies included and the highly questionable interpretations of rare events, there’s an even bigger issue that jumped right out at me when I read the Materials and Methods section, where they described their search strategy for their scoping review:
A comprehensive search of the world’s literature was conducted using PubMed, Scopus, Web of Science, Google Scholar, and React19 between January 2020 and April 2025. Eligible publications included case reports, case series, cohort or population-level analyses, systematic reviews, and mechanistic or preclinical studies that described either (i) new-onset, recurrent, or rapidly progressive malignancy temporally associated with COVID-19 vaccination or SARS-CoV-2 infection, or (ii) experimental evidence implicating vaccine or infection-induced immune perturbations in oncogenic, proliferative, or metastatic processes.
Initial searches in PubMed using conventional keyword combinations such as “COVID-19 vaccine and cancer,” “vaccination and cancer,” “COVID-19 vaccine and tumor,” or cancer-specific terms paired with “COVID-19 vaccine” yielded little to no indexed results. Even when known case reports were used as anchors for “similar articles,” PubMed returned no related entries. This highlighted a structural limitation in standard indexing pathways and necessitated a broader, more strategic search approach.
Wait, what?
React19.org is a valid data source? I don’t think so
I basically facepalmed when I read that Kuperwasser and El-Deiry were including React19.org in their search strategy, along with more traditional databases like PubMed, Scopus, Web of Science, and Google Scholar? Notice how they justify including React19 because they didn’t find enough references searching PubMed using conventional keyword combinations related to vaccines and cancer. Let me just note that React19 is a highly dubious source, maintained by an organization that proclaims its purpose thusly:
React19 is a science-based non-profit offering financial, physical, and emotional support for those suffering from longterm Covid-19 vaccine adverse events globally.
Our mission is to bring healing to the moms, dads, friends, and loved ones who are facing life-altering side effects from their Covid-19 vaccine. We build bridges between patients and research institutions in order to develop a better understanding of our vaccine complications. React19 works with both patients and providers, as well as research teams. Our programs all fall within our 3 categories of assistance (financial, physical, and emotional). Programs include funding, promoting, and sharing relevant scientific research; bringing the right medical teams together with patients; direct financial assistance; educational outreach; and supporting communities where impacted people can begin to heal physically and emotionally.
I examined React19.org’s X feed and soon found that it sure looks like an antivax org, full of anecdotes of alleged horrific injuries due to COVID-19 vaccines, even to the point of platforming longtime antivax activists like Dr. Sherri Tenpenny:
suppressing the evidence regarding vaccine injuries, you’re antivax.
Right from the start, Dr. El-Deiry’s approach appears to be: If he can’t find articles damning COVID-19 vaccines from standard databases of biomedical research articles, he’ll look elsewhere, even if he has to turn to a source that is clearly antivax. If I were reviewing his manuscript, his inclusion of React19.org would have been enough, in and of itself, for me to strongly recommend rejecting the manuscript with extreme prejudice.
Epidemiological evidence for a COVID vaccine-cancer link? Not so much…
Kuperwasser and El-Deiry clearly want the reader to think that there is a cancer safety signal in epidemiological data. The problem is that the studies that they cite don’t really show that, at least not anywhere near convincingly. They all have serious confounders that can explain their results. One study in particular cited by Kuperwasser and El-Deiry stood out to me very strongly, mainly because I have discussed it before—and fairly recently. I’m referring to the Korean study that was being widely touted a few months ago as slam-dunk evidence that COVID vaccines are associated with an increased risk of cancer, which Kuperwasser and El-Deiry describe thusly:
Kim et al. [8] analyzed approximately 8.4 million individuals between 2021 and 2023 to assess 1-year cumulative cancer incidence following COVID-19 vaccination using the South Korean National Health Insurance Service database. The authors reported statistically significant associations between vaccination and six specific cancers, including thyroid (HR 1.35), gastric (HR 1.34), colorectal (HR 1.28), lung (HR 1.53), breast (HR 1.20), and prostate cancer (HR 1.69) using propensity score matching and multivariable Cox proportional hazards models. Associations varied by vaccine platform, with mRNA vaccines linked to thyroid, colorectal, lung, and breast cancers, and cDNA/adenoviral vaccines associated with thyroid, gastric, colorectal, lung, and prostate cancers; heterologous vaccination was associated with thyroid and breast cancer. Stratified analyses suggested effect modification by sex and age, and booster-dose analyses identified increased risks for gastric and pancreatic cancer. The authors emphasized that despite adjustment for measured confounders, residual confounding, detection bias, and limited follow-up preclude causal inference, and that the findings should be interpreted as epidemiologic associations warranting further study rather than evidence of vaccine-induced cancer risk.
I deconstructed the study in depth not long after it was published; so I won’t go into great detail here. Suffice to day that this study, carried out in South Korea, screamed healthy vaccinee bias at me, given that it only looked at cancers diagnosed at one year. You might recall that healthy vaccinee bias is a type of confounding in observational studies (like this one, a retrospective observational study) where healthier, more health-conscious individuals are more likely to get vaccinated. This bias can lead to the overestimate of vaccine efficacy, which is obviously not an issue in this study, which didn’t even try to estimate vaccine efficacy. That wasn’t its purpose. Healthy user bias, which is related, is the likelihood that people engaging in one health behavior (e.g., getting vaccinated against COVID-19) will be more likely also to engage in other health interventions, such as cancer screening. What the results of the S. Korean study finding increased cancer diagnoses in vaccinated people seemed to be far more compatible with was a failure to correct for screening intensity, along with other potential confounders, so that the likelihood that people who were vaccinated and boosted were more likely to undergo screening, leading to an apparent increased incidence of the six screen-detected cancers described within a year, or to seek medical care for lesser symptoms, leading to, for instance, an earlier diagnosis of pancreatic cancer, a cancer that is not routinely screened for.
Kuperwasser and El-Deiry also cite an Italian study that was represented as finding increased rates of hospitalization for cancer in patients who had been vaccinated but suffers from much the same problems. Indeed, the authors themselves note:
Compared with the unvaccinated, those receiving ≥1 dose showed a significantly lower likelihood of all-cause death, and a slightly higher likelihood of hospitalization for cancer (HR: 1.23; 95% CI: 1.11-1.37). The latter association was significant only among the subjects with no previous SARS-CoV-2 infection, and was reversed when the minimum time between vaccination and cancer hospitalization was set to 12 months. The subjects who received SARS-CoV-2 vaccination showed a substantial reduction in all-cause mortality, and a risk of cancer hospitalization that varied by infection status, cancer site, and the minimum lag-time after vaccination. Given that it was not possible to quantify the potential impact of the healthy vaccinee bias and unmeas-ured confounders, these findings are inevitably preliminary.
This was not at all convincing for a link between COVID vaccination and cancer, and even Kuperwasser and El-Deiry seem to realize this, noting:
Both studies provide early, population-level associations rather than causal estimates and underscore the importance of long-term follow-up and molecular correlation to distinguish true biological effects from health-system or behavioral confounders.
The problem is that neither study actually shows a convincing population-level association after proper control for very obvious confounders, nor does the Department of Defense study cited, which showed an increase in incidence among military personnel of mature T/NK-cell lymphomas that began in 2020 (before vaccines) and continued through 2021-2023 (after military personnel were almost universally vaccinated against COVID-19). Even Kuperwasser and El-Deiry were forced to concede, however, that the “authors did not attribute the observed changes in NHL [non-Hodgkins lymphoma] incidence to vaccination or infection,” and that “the analysis was not designed to establish causality at the individual level,” noting that changes “in diagnostic practices, healthcare access and utilization, and pandemic-related disruptions to routine medical care cannot be excluded from this time-trend analysis as with others conducted during the pandemic period.” Of course, none of this prevents them from speculating wildly that “population-level analyses combined with the case-based literature indicate that a cancer signal warrants further prospective evaluation to determine whether COVID-19 vaccination confers any measurable cancer risk or merely reflects surveillance and reporting biases.”
Oddly enough, what is written above is a lot more tame and tentative than what Dr. El-Deiry said to CHD when he said that the thought these signals were a “smoking gun.” It’s as though Dr. El-Deiry cloaks the conclusions of his scientific articles in all the caveats expected but lets his real beliefs out when talking to antivax outlets like CHD. It’s almost as if Dr. El-Deiry knows that he’s generating material for antivaxxers to weaponize against vaccines. This is a recurring theme when comparing the actual review article and what Dr. El-Deiry says about it on social media and in interviews. (Seriously, Dr. El-Deiry, please stop promoting your results to loons like those working at CHD, thus giving them fodder for their antivax propaganda and lending your name to it as well. I honestly care less that you seem to think this really weak evidence is some sort of super-concerning “cancer signal” that requires further investigation than that you seem to be enthusiastically participating with antivaxxers who want to weaponize your findings to cast doubt on vaccines.)
DNA contamination a-go-go!
Moving on, Kuperwasser and El-Deiry really lose the plot when they discuss the issue of “DNA contamination” of COVID-19 mRNA vaccines. Recall that one of the tenets of the belief system behind “turbo cancer” is that there is a large amount of residual DNA contamination in the vaccines left over from the plasmids used to make the vaccine that the SV40 promoter sequence. I’ve discussed time and time again just how implausible this is and how bad the studies claiming to find high levels of DNA contamination in the vaccines are. Does any of this stop Kuperwasser and El-Deiry from citing the same crap studies, by the likes of Kevin McKernan and Didier Raoult? Of course not. It didn’t even stop him from citing a publication from Science, Public Health Policy, and the Law, the antivax fake journal founded by James Lyons-Weiler and published by his antivax org the Institute for Pure and Applied Knowledge (IPAK), which, in addition to publishing poor quality antivax studies, also launders retracted studies by antivaxxers by finding a new home for them that appears to be a legitimate journal. Tellingly, Kuperwasser and El-Deiry don’t even cite a recent high quality paper that basically concluded that prior claims of excess DNA contamination of the vaccines was due to misinterpretation of improperly conducted analyses—ouch, that’s got to hurt—and that, in reality, DNA contamination of the Pfizer and Moderna vaccines is well below accepted safety limits when the specimens are subjected “rigorous application of well-controlled methods that minimise mutual interference of vaccine components.” (Ouch. That’s going to hurt more.)
I could go on and point out how, even if the DNA contamination were as horrendous as McKernan (and, apparently, Kuperwasser and El-Deiry) want you to believe, it would still be incredibly unlikely even for piece of DNA containing an intact SV40 promoter to cause cancer. First, it would have to get into the nucleus, which naked DNA has a hard time doing. Second, it would have to integrate into the genome in just the right spot that either (1) turns on a powerful oncogene or (2) disrupts a powerful tumor suppressor gene. Even if you accept the estimate provided in the paper based on in vitro (cell culture) studies as valid in vivo (in the human body) that 1-10% of cells demonstrate genomic integration of DNA with lipid-based systems, the only location where the concentration of such DNA contamination, even if you accept the highest estimates, might accomplish that is the muscle injection site, and that would mean the only sort of cancer that might even theoretically be caused by such a mechanism would be a soft tissue sarcoma arising from the muscle or connective tissue. None of this stops Kuperwasser and El-Deiry from writing, “No studies have been conducted demonstrating that the level of DNA impurities present in the vaccines are insufficient to transfect cells, nor have studies ruled out the possibility of integration.”
Prove to me a negative! (Dr. El-Deiry should know that science can’t absolutely prove a negative.)
The review does include a case report of an injection site sarcoma—one case report. You’d think that if DNA contamination were such an issue and if COVID-19 vaccines were responsible for “turbo cancer”—excuse me, “hyperprogression,” as the authors prefer to call it—there would have been a lot more such cases in the literature after billions upon billions of doses of vaccine. I can’t totally discount the possibility that an mRNA-based COVID-19 vaccine was responsible for this woman’s sarcoma near her injection site, but even if it was the lack of more cases suggest that such an event is so incredibly rare as to be almost undetectable epidemiologically. Such a conclusion conflicts with the “turbo cancer” narrative, in which antivaxxers are claiming that vaccines are responsible for a wave of highly aggressive cancers, even though there is no evidence of such a wave and the evidence for an increase in cancer among younger people shows that the increase started over three decades before the pandemic.
But, biology, man!
There is a whole section of the paper that tries to argue for biological plausibility based on mainly in vitro studies, for a couple of hypotheses. One is that the spike protein itself can cause cancer through a variety of biological activities. Perusing the list of articles cited to support this contention I was struck how most of them were looking at SARS-CoV-2 infection rather than vaccination. (Remember my discussion of speculation in 2024 that SARS-CoV-2 infection might predispose to cancer?) You might remember that Dr. El-Deiry himself published articles suggesting that the spike protein might bind to the p53 (TP53) tumor suppressor gene and thereby predispose to cancer, writing:
The transformation of a normal cell into a cancer cell involves disruption of multiple safeguards controlling cell growth, survival, and DNA repair. Laboratory studies have reported that the spike protein, whether it is produced by infection or by vaccination, has biological activities [110, 145, 152–158] with oncogenic potential [159–161]. For example, in addition to interacting with ACE2 receptors, spike protein fragments have been shown to interact with NRP-1, integrins, and TLRs leading to VEGF/NRP-1 signaling [155, 162, 163]. Spike protein has also been reported to induce DNA damage [160, 164, 165] and modify p53 pathway under oxidative stress [164, 166]. Therefore, in theory, such interactions of spike protein with these pathways could contribute to cellular transformation, both from the vaccine but also from infection, especially if the spike protein remains present long after vaccination or from multiple COVID infections.
The problem is that this is highly speculative. Indeed, the phrase “in theory” is doing some seriously heavy lifting here. As I read this, I asked myself one question: Has anyone demonstrated that the spike protein can transform cells, even in vitro? Nope. Not that I’m aware of. Until I see that, I will give this speculation all the due that it deserves; i.e., brief consideration before demanding some actual direct data.
Another hypothesis in the review is that the vaccine somehow causes immune dysregulation that leads to the growth of the latent cancer cells that we all have in our bodies that are generally kept in check by our immune systems. Let’s start with that one:
The rapid appearance of cancer, the anatomical proximity of the tumors to vaccine sites, and the histologic signatures of inflammation the support immune mechanisms that promote the progression of latent clones rather than de novo carcinogenesis. We hypothesize two interrelated processes: localized inflammation and modulation of the tumor microenvironment with transient functional immunosuppression that relaxes immune surveillance. Might account for hyperprogression of latent or occult cancer cells (Figure 5).
Accompanying this is a diagram that illustrates a “conceptual model” for the proposed mechanism:
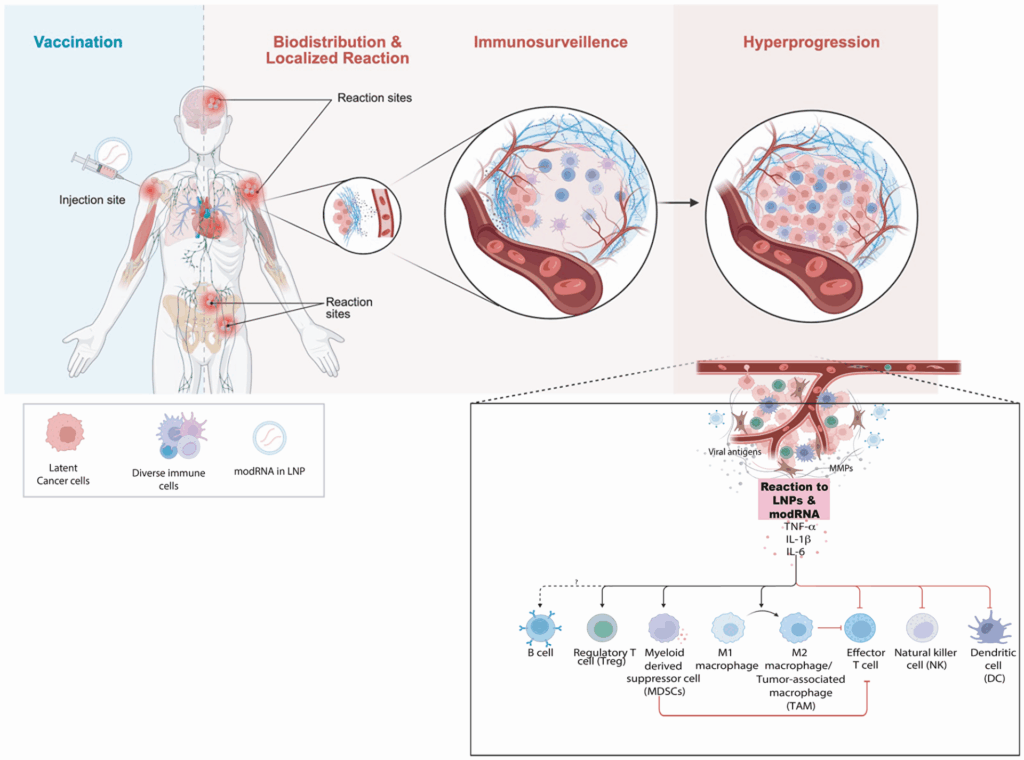
I’m not an immunologist, but you don’t have to be an immunologist to I recognize this as handwaving of the first order. Let me just briefly show you what I mean. The overall argument being made is that there’s a transient cytokine surge after vaccination against COVID-19 that can cause secretion of proteins known as cytokines that lead to a “synergistic pro-inflammatory circuit capable of stimulating proliferation and angiogenesis” that is “known to rapidly promote the development of cancer if transformed or pre-malignant cells already exist.” Here’s one thing. Some articles cited implicate mainly chronic inflammation as a trigger for activating dormant tumor cells, while others implicate more acute inflammation, while one cited article is about respiratory infections activating breast cancer metastases in lungs, concluding that “SARS-CoV-2 infection substantially increases the risk of cancer-related mortality and lung metastasis compared with uninfected cancer survivors.” (Vaccinating would be a good way to prevent that.)
Here’s the other thing. All vaccines cause a transient cytokine surge. That’s how they work! They provide an antigen (± adjuvant) that results in stimulation of the immune system and, ultimately, immune memory of the antigen, so that the immune system is ready to be more rapidly activated if it ever encounters the same antigen(s). Why, then, would Kuperwasser and El-Deiry focus solely on COVID-19 vaccines as potentially causing a brief inflammatory cytokine storm that can cause dormant tumor cells to activate and start growing rapidly? Inquiring minds want to know, and certainly no explanation is given in the paper as to why COVID-19 vaccines would be more likely to cause this phenomenon than, basically, any other vaccine in existence.
Then there was one final thing about the immune system. Remember that study I discussed a couple of months back in which it was shown that mRNA vaccination with COVID-19 vaccines is associated with higher rates of survival in patients with advanced cancers undergoing immunotherapy with immune checkpoint inhibitors such as pembrolizumab? It’s dismissed by the authors by saying that, “mRNA vaccination was associated with increased Type I interferon signaling and elevated tumor PD-L1 expression” but that “PD-L1 upregulation in the absence of checkpoint inhibitor therapy is generally associated with enhanced tumor immune evasion and resistance to T-cell–mediated cytotoxicity, raising questions about the biological interpretation of these findings.” How? They don’t really say, but they go on to say that “the study did not provide comparative analyses between interferon treatment and the combination of mRNA vaccination with checkpoint blockade,” which would have been nice but doesn’t really detract from the study’s findings. They also write:
Furthermore, the study did not address key limitations, alternative mechanistic explanations, or the broader clinical context necessary to fully interpret the reported effects.
Personally, I thought that the authors of the immune checkpoint inhibitor (ICI) study did these things just fine. For instance, the authors looked at patients who had received non-mRNA-based vaccines, like the influenza vaccine, within 100 days of their immunotherapy and found no survival benefit, and they did discuss potential other mechanisms and also basically replicated in mice what they had observed in the retrospective study and (2) using a different antigen (in this case, the cytomegalovirus antigen pp65, which is expressed in in human glioma but not in B16F0 tumors) they showed similar results, with the addition of mRNA vaccine to ICI therapy resulting in more potent anti-tumor effects.
Near the end of the article, there’s a section called “Gaps in Knowledge.” I hate to say it, but this is basically an appeal to ignorance combined with a Gish gallop to give the impression that we know so little about how spike protein from SARS-CoV-2 or the vaccine causes cancer, without any actual evidence that the spike protein from SARS-CoV-2…oh, you know…actually causes cellular transformation or cancer, which is why I cringed when I read:
The distinction between vaccination associated tumor initiation and promotion also remains unresolved. There is no empirical validation that vaccination only accelerates pre-existing disease rather than also initiating new malignancies.
This is as perfect an example of putting the cart before the horse. There is no good evidence that COVID-19 vaccination causes new malignancies or accelerates pre-existing disease; certainly nothing but speculation based on carefully selected articles was presented in this review article, and even then the case presented was not very persuasive.
Then there are errors. So. Many. Errors. The entry on the review article on PubPeer—oh, dear, I hope I don’t anger Dr. El-Deiry too much—goes into them in great detail; so I’m not going to enumerate them all. I will point out one, however:
“Notably, a study of cardiac tumors in the post-COVID period revealed both a 1.5% increase in tumor incidence and the expression of spike protein with the tumors, particularly in those associated with vaccination [86].” However the authors of the referenced paper by Mitrofanova et al. (2023) state: “There was no correlation with vaccination, and no significant differences were found between patients from 2016–2019 and 2021–2023 in terms of gender, age, and cardiac rhythm disorders”. Either this article was misinterpreted by the authors, or was cited incorrectly.
I tend to think it was misinterpreted.
But what about React19.org again?
I mentioned early in this post that Kuperwasser and El-Deiry had included React19.org, an antivax organization, in its data sources. However, if you look through the article, it’s hard to figure out where React19.org even comes in. For that, I had to look to the peer review. Oddly enough, Reviewer #1 didn’t even mention the very obvious problem that including data from an antivaccine group that isn’t even curated or subject to peer review as if it were co-equal with publications from sources such as PubMed and Google Scholar, while the best Reviewer #2 could come up with was:
The authors indicate that most of the oncologic effects were associated with vaccination. Could this be due to the inclusion of REACT19 in their database search?
Not the greatest question. I would have asked what the heck the authors were thinking when they included a database maintained by an antivax organization, but at least someone asked about React19.org. In any event, I assume that what was included was this listing of 3,500 publications supposedly related to COVID-19 adverse events, of which 199 fall under the category of “oncology.” Perusing the list, I noticed that a lot of the articles involved lymphadenopathy in nearby nodes to the injection site and how they can confound the mammographic diagnosis of breast cancer, something known since soon after the vaccines rolled out. In any event, the authors responded:
Yes, the REACT19 database was one of several resources used in our search strategy, and when filtered for “Oncology” it contains approximately 199 references. Many of the reverences overlap with the peer-reviewed literature identified through PubMed, Scopus, Web of Science, and Google Scholar but could not be found using conventional searching on those platforms.
Thus, the rationale for including REACT19 was not to preferentially capture vaccine- associated outcomes, but rather to address a well-recognized limitation in the discoverability of peer-reviewed publications on SARS-CoV-2 infection, COVID-19 vaccination, and cancer. As noted in the Methods and Limitations sections, much of the relevant literature is not consistently indexed with standard Medical Subject Headings (MeSH) or cross-referenced using conventional oncology or vaccinology search terms. Consequently, reliance on traditional database queries alone fails to retrieve a substantial portion of the existing peer-reviewed case literature.
We explicitly acknowledge in the manuscript that this reliance on publicly available but incompletely indexed literature imposes inherent limitations, including potential reporting bias, incomplete capture, and challenges in verification. We emphasize that this affects both infection- and vaccination-associated reports and reflects structural limitations of current indexing systems rather than an a priori focus on vaccination. Accordingly, the predominance of vaccination-associated reports in the assembled literature should be interpreted as descriptive of the published record to date, not as evidence of differential risk.
I would be interested in discovering which studies could not be found using conventional searches of PubMed, Scopus, and Google Scholar, but were found only in the much smaller React19.org database. Inquiring minds want to know, and I must admit that I’m not willing to take the time to try to duplicate all the searches that the authors list in their methods. Looking at the list of 199 references at React19.org, I doubt now that including the database made much of a difference, but the fact that the authors don’t recognize that they were using a database maintained by an antivax source disturbs me.
Mixed messages drive me crazy
Overall, this review article is basically a nothingburger. It’s far more speculation than anything else, as I mantioned before, a case of putting the cart before the horse. The authors carefully select three studies that they think they can point to as strong suggestive evidence in population studies that COVID-19 vaccination is associated with an increased risk of cancer. When these studies are examined in more detail, they all suffer from potential confounders that could easily explain their results, none more than the S. Korean study, which is about as obvious an example of healthy user/healthy vaccinee bias as I’ve ever seen. The authors also present a tiny number of case reports—at least the number is incredibly tiny relative to the billions upon billions of doses of vaccine that have been administered over the last four years—as though they suggested anything but the entirely predictable phenomenon that, if you administer a medication to a large enough number of people, you will find a number of bad things that happen to a number of people soon after receiving that medication by random chance alone. No convincing argument or evidence is presented to suggest causation.
Next, they list various mechanisms by which COVID-19 vaccines in general—and the spike protein in particular—might cause cancer. They then speculate wildly about these potential biological mechanisms and “gaps in knowledge” about COVID-19 vaccines and cancer. Most of these biological mechanisms strike me as a stretch, at best, particularly the invocation of “inflammation” as somehow activating dormant cancer cells that we all have in our bodies, again, because all vaccines cause transient inflammation, but the authors don’t address what is different about the inflammation caused by COVID-19 vaccines that it would lead to cancer.
There’s just one problem. If COVID-19 vaccines were truly responsible for a wave of “turbo cancers” or, as the authors would prefer to say, hyperprogression, then the epidemiological data would be there now, and it would be impossible to deny. By now, there would have been a worldwide wave of cancer correlating temporally and physically with the rollout of COVID-19 vaccines across the globe. We see no such thing. Related to this problem is the paucity of evidence that COVID-19 vaccines or the spike protein generated by them can cause neoplastic transformation (conversion of a normal cell to cancer) in cell culture or animal models, much less in humans. Again, this whole review article strikes me, more than anything else, as an exercise in—you guessed it!—putting the cart before the horse. Seriously, provide us with some compelling evidence, and we will change our minds, but Kuperwasser and El-Deiry don’t because they can’t. That evidence doesn’t exist, and it isn’t for lack of people trying to find it, either.
The mixed messages this review gives are best summed up by comparing the Limitations section to the conclusion of the paper. The authors list limitations such as:
The findings of this review should be interpreted within several important limitations inherent to the available literature and study design. First, although there are larger studies published, most reports are single-patient case descriptions or small case series. Many reports lack documentation of pre-existing conditions, prior oncologic history, concurrent infections, or medications that could confound interpretation. Therefore, while these observations are valuable for early signal detection, they are highly susceptible to publication bias and selective reporting. It is plausible that cases perceived as unusual or temporally linked to vaccination are preferentially submitted for publication, while the absence of comparable control observations limits inference regarding incidence or relative risk.
Let’s also not forget to emphasize yet again that, compared to the billions of humans who have collectively received billions of doses of vaccine, the number of these cases is mind-bogglingly infinitesimal, leading to the more likely possibility that many, if not all, of these case reports represent coincidence, a possibility not even really considered seriously by the authors.
Then:
The mechanistic hypotheses proposed here remain speculative in the absence of direct in vivo validation. No current studies have demonstrated oncogenic transformation or tumor initiation causally attributable to the COVID mRNA vaccine or its components. Nor have animal studies demonstrated vaccine-induced tumor promotion either. These mechanisms should therefore be regarded as biologically plausible models that warrant targeted experimental study.
This argument is basically: Ignore the lack of evidence supporting any of our speculations. We still think these biological mechanisms are plausible, and you should too, so much so that you should take our conclusions seriously:
The collective world-wide evidence from 2020–2025 underscores a biologically plausible connection between COVID-19 vaccination and cancer. The recurring clinical findings documented across many reports of de-novo cancer onset, rapid tumor progression, viral reactivation, and reawakening of dormant disease, highlight critical gaps in knowledge and understanding of how large-scale immune changes produced by the vaccine interacts with cancer biology.
Except that the whole review article is basically forced to admit that the collective worldwide evidence from 2020-2025 does not actually “underscore a biologically plausible connection between COVID-19 vaccination and cancer.” If it did, there would be at least some direct and compelling evidence implicating COVID-19 vaccines and cancer. There isn’t. Even Kuperwasser and El-Diery are forced to admit it.
So what happened to Dr. El-Deiry? He’s been in science longer than I have. By any objective measure, he’s accomplished way more in his scientific career than I have, with close to ten times the number of publications that I have, and even though his first publication was seven years before mine that doesn’t explain such a huge difference. Dr. El-Deiry also did pioneering work on both p53 and on p21 and is now the director of a major cancer center. In contrast, as I enter the home stretch of my career, I know that I will never be a cancer center director or even a chair of a department of surgery. Yet, for some reason, late in his career, Dr. El-Deiry has embraced contrarianism. Worse, he’s embraced conspiracism to the point of trying to get the attention, well:
Let’s just say that snitch-tagging antivaxxers like RFK Jr., Dr. Peter McCullough, and the anonymous Jikkyleaks is not a good look for any scientist, no matter how much under attack he feels himself to be.
I keep scratching my head and trying to give Dr. El-Deiry the benefit of the doubt. His incredible past scientific accomplishments, coupled with my previous admiration for his work, compel me. But I’m having a harder and harder time managing to continue doing it, particularly now that he’s published an article that uses classic techniques that I’ve long watched antivaxxers use for two decades, specifically citing all sorts of scientific studies and engaging in imaginative speculation about “mechanisms” of vaccine injury, all without actually showing any compelling scientific evidence that the vaccine injury postulated is actually occurring. In such reviews, the tentative nature of scientific discourse is maintained, but the articles serve primarily to cast doubt on the safety and efficacy of a vaccine (or vaccines). It’s difficult for me not to see this article the same way, particularly given that Dr. El-Deiry is now portraying himself as the victim of persecution and conspiracy based on the criticism, sometimes harsh, of his claims about COVId-19 vaccines.