{kind=link}
 In the tradition of James Randi, a Chinese doctor who is an outspoken critic of Traditional Chinese Medicine (TCM) has issued a challenge to its proponents. He has put up 50,000 yuan (about $8,000), which has been matched by donors for a total of over 100,000 yuan, to any TCM practitioner who can use pulse diagnosis to determine with accuracy whether females subjects are pregnant.
In the tradition of James Randi, a Chinese doctor who is an outspoken critic of Traditional Chinese Medicine (TCM) has issued a challenge to its proponents. He has put up 50,000 yuan (about $8,000), which has been matched by donors for a total of over 100,000 yuan, to any TCM practitioner who can use pulse diagnosis to determine with accuracy whether females subjects are pregnant.
Ah Bao is the blogging pseudonym of a burn-care doctor at Beijing Jishuitan hospital. He is trained in scientific medicine and has criticized his country for clinging to pre-scientific philosophy-based health care. He calls TCM “fake science” and now wants to demonstrate that the claims of TCM practitioners are without factual basis.
His challenge is a good one because it focuses on a clear criterion. Subjects will either be pregnant or not pregnant, and the TCM practitioner, using only pulse analysis and blinded to the patient themselves, must determine with an 80% accuracy which subjects are pregnant. A TCM practitioner, Zhen Yang, has taken him up on the challenge and they are now working out the details.
Pulse analysis
Scientifically-trained doctors do palpate peripheral pulses as part of the medical exam. We look for the strength, rhythm, and rate of the pulse, compare right-left symmetry and look for the presence of specific pulses. The purpose of examining the pulse is to help evaluate the cardiovascular system. An irregularly irregular pulse would indicate atrial fibrillation. A weak pulse could indicate dehydration, heart failure, or hemorrhage (essentially low blood pressure).
TCM pulse analysis, however, is different. It’s possible that some of the basic physiological phenomena above were recognized even by pre-scientific practitioners. It’s not a stretch to realize that a weak pulse indicates the patient is not healthy. But they had no real understanding of cardiovascular physiology, autonomic function, or cardiac electrical activity. Instead they developed an elaborate scheme relating various properties of the pulse to concepts within TCM.
Here is a description of the 29 pulses of TCM, with a notation about their cause and in places relating to a biological etiology. For example a “hesitant” pulse indicates, “Blood and essence failing to nourish the meridians. Blood is not flowing smoothly.” Whereas a “wiry” pulse indicates: “Tense vascular Qi due to the liver not gently performing its function, can also be due to the retention of a pathogen in the liver. If wiry, Thready [sic] and forceful-like feeling the edge of a knife is indicative of Stomach Qi exhaustion.” Most of the descriptions relate to the Yin and Yang of Chi.
None of this has any basis in our modern understanding of biology or medicine. It is clearly the attempt of a pre-scientific culture to impose an elaborate system onto a complex and mysterious phenomenon.
Disconnected from reality
Pulse diagnosis and other similar aspects of TCM are, in my opinion, an excellent example of what happens when “knowledge” is disconnected from reality. The scientific method is primarily about creating a feedback loop in which our ideas are tested in some objective and systematic way against reality. Without this feedback loop, our ideas are free to drift into any direction. Historically the lack of scientific testing has resulted in elaborate and fanciful systems of pretend knowledge. Humans are creative and inventive, and so we have no difficulty imagining and embellishing such systems. Confirmation bias then convinces us that our systems are real.
There are countless examples of this phenomenon. The many forms of astrology, for example, represent pretend knowledge. Galenic medicine, based on the notion of the four humors, was the Western version of fake medical knowledge. In fact, bloodletting and the balance of the humors in the West was culturally connected to acupuncture and cupping (which actually were forms of bloodletting) and the balance of Chi in the East. These were actually different versions of the same basic ideas.
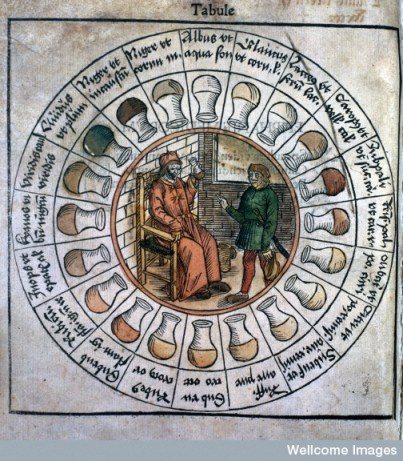
Another elaborate diagnostic system disconnected from reality was diagnosis by urine color. Medieval doctors would carefully examine their patient’s urine for color, odor, and even taste and had a complex system of diagnosis. As with pulse diagnosis, there are legitimate clues to health that can be gleaned from the urine, but only in specific situations.
Medieval doctors, however, without the knowledge or technology to truly understand what was going on with their patients, grasped onto whatever was available. They developed elaborate charts, like the one here, relating the subtle variations in urine color to specific (but also largely fictitious) conditions. This is a perfect analogy to pulse diagnosis.
Pretend knowledge is very dangerous because it can create the powerful illusion of genuine knowledge. Confirmation bias is a persistent and subtle bias in the way we perceive, filter, and evaluate information that systematically supports what we already believe or wish to be true. It largely occurs without our conscious awareness. We also tend to be unaware of the vast amounts of data we are sifting, and so when we find bits of data that seem to support our beliefs we find it unlikely that there is an alternate explanation.
In medicine there are other factors that also conspire to create the powerful illusion that even entirely fake beliefs are legitimate. Chief among these factors are placebo effects – effects that make it seem as if a treatment is having a benefit even when it is doing nothing. Placebo effects are largely illusory, such as regression to the mean (symptoms getting better as a matter of course).
There are other factors as well, such as the tendency to only test our own hypothesis rather than competing hypotheses. This is often referred to as the toupee fallacy. It is easy to have the illusion that you always recognize when someone has a toupee, because you don’t test the hypothesis when you don’t recognize a toupee. Likewise, when taking a medical history you might preferentially ask the patient questions which are designed to confirm your diagnosis, rather than questions that will challenge the diagnosis.
For example, if you think that a “soggy” pulse is associated with breathing problems, and you feel as if you detect a soggy pulse, you might ask the patient about breathing problems and will take the fact that many patients respond positively as confirming the reality of the “soggy” pulse and its association with breathing problems. But what if you asked all your patients if they had breathing problem, regardless of their pulse? Would the percentage who answers in the positive be any different? That is the difference between science and confirmation bias.
Unsurprisingly, the reality of pulse diagnosis has not been established by scientific evidence, any more than medieval urine analysis or the four humors. There are a few studies looking at pulse diagnosis but they amount to what Harriet cleverly termed “tooth fairy science.” They study aspects of pulse diagnosis without ever doing the kind of test that would establish whether or not it is valid. For example, there is a study attempting to standardize the position of the fingers when sensing the pulse.
Another study correlated how TCM practitioners describe the pulse to the presence or absence of hypertension. This study is problematic in a number of ways. First, hypertension might actually affect the pulse and therefore its description, and so is a problematic model for TCM pulse diagnosis in general. Further, it committed, essentially, the toupee fallacy of only testing the desired hypothesis but not testing this against controls that could disprove the hypothesis.
“Tooth fairy science” takes a fake belief system and transforms it into a pseudoscience by going through the motions of scientific analysis, but only as a more elaborate form of confirmation bias. This makes the fake belief system more dangerous because it gives it the patina of science and therefore false respect and legitimacy.
Conclusion
I agree with Ah Bao that there is no scientific legitimacy to TCM generally and pulse diagnosis specifically. It is, as he says, “fake science.” It is just one more example of what happens when beliefs are disconnected from reality – elaborate and detailed, but entirely fictitious, belief systems emerge.
I look forward to following the development of the pulse diagnosis challenge. Hopefully Ah Bao is experienced enough to design and execute a study that precludes any form of “cheating” or inadvertent information leakage.
It’s not physiologically impossible that the radial pulse is systematically different in pregnant vs non-pregnant women. The pulse, as I mentioned above, is a real physiological phenomenon. I doubt, though, that any such signal will be consistently detected among the noise of all the other factors that affect pulse. I would expect, therefore, that the test, if properly controlled and sufficiently powered, would be negative. Either way the results will be interesting.
Usually more interesting than the outcome of such challenges are the responses of believers to the outcome.