{kind=link}
One of the disadvantages of writing for this blog is that sometimes I feel as though I spend so much time deconstructing bad science and pseudoscience in medicine that I’m rarely left with the time or the opportunity to discuss some interesting science. Of course, even when I do that, usually it’s in the context of that very same bad science or pseudoscience, and this post won’t be different. Still, there was some interesting science with respect to vaccines published last week in Science, and I think it’s worth looking over. The only thing that surprises me is that the antivaccine movement hasn’t jumped all over it yet. On the other hand, its press coverage was relatively minimal, and I didn’t really notice it until an article appeared on (sadly, yes) The Huffington Post entitled “The Measles Vaccine Can Protect Against Much More Than Measles, According To New Study“:
A new study suggests the measles shot comes with a bonus: By preventing that disease, the vaccine may also help your body fight off other illnesses for years.
It’s long been known that contracting measles weakens the immune system for weeks or months, putting people, especially children, at increased risk for potentially fatal infection by a host of germs.
Now, scientists find that this vulnerable period goes on much longer than thought, up to three years. So the benefit of avoiding measles also extends longer than was appreciated. Researchers also found that measles vaccination campaigns were followed by a drop in deaths for other infectious diseases.
Experts said the work is a wake-up call to parents who don’t vaccinate their children out of unfounded fears about a link between vaccines and autism.
Or, as is reported in more detail in this NPR story, this is what happened after the introduction of measles vaccination campaigns:
Childhood deaths from all infectious diseases plummeted. Even deaths from diseases like pneumonia and diarrhea were cut by half.
Scientists saw the same phenomenon when the vaccine came to England and parts of Europe. And they see it today when developing countries introduce the vaccine.
“In some developing countries, where infectious diseases are very high, the reduction in mortality has been up to 80 percent,” says Michael Mina, a postdoc in biology at Princeton University and a medical student at Emory University.
“So it’s really been a mystery — why do children stop dying at such high rates from all these different infections following introduction of the measles vaccine,” he says.
Of course, as I’ve discussed on many occasions, before the introduction of the measles vaccine in the early 1960s, there were routinely a half a million cases of measles per year in the US, an incidence that dropped dramatically, as shown on this graph, which I’ve used periodically whenever I want to make this point:

Also each year, out of those roughly a half million cases, an estimated 400 to 500 people died, and there were around 48,000 hospitalizations, with 4,000 ending up suffering encephalitis (swelling of the brain) from measles. Contrary to antivaccine activists invoking what I like to refer to as the “Brady Bunch” fallacy, a name I chose based on how antivaccinationists like to invoke a 1969 episode of the Brady Bunch in which all six children, the father, and the maid Alice came down with the measles, a situation that was played for laughs. In the episode, the measles was portrayed as no big deal, a normal childhood disease that almost everyone gets, and the kids were shown happily playing board games and rejoicing that they got a few days off from school. The message? Obviously that the measles shouldn’t be feared. But it should. As Clay Jones reminded us not too long ago, the most feared and deadly complication of measles, subacute sclerosing panencephalitis (SSPE) is not as rare as it is portrayed, and after a measles infection it can appear after a latent period lasting 6-8 years to cause an encephalitis that kills most children it affects within three years. Actually, SSPE is rare now, but that’s because its incidence plummeted after widespread measles immunization efforts caused the incidence of measles to plummet. As Clay put it, where there is more measles, there is more SSPE.
All of the above observations are more than adequate reasons to immunize against measles. However, if the recent study in Science is correct, measles vaccination is even more important than the reasons above make it because it prevents more than just measles. Let’s take a look at the study by Mina et al. out of the laboratory of Bryan T. Grenfell, “Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality“, the study that spawned the stories I cited above. It’s a study funded by the Bill and Melinda Gates Foundation that comes out of the Department of Ecology and Evolutionary Biology, Princeton University; Emory University; the Fogarty International Center at the National Institutes of Health; and the Department of Viroscience, Erasmus University Medical Center, Rotterdam, Netherlands. Not only does it provide a possible answer to one of the great mysteries of measles and the measles vaccine, but it suggests that measles vaccination is even more important than it is already known to be. The reason is as described in the stories above, introduction of mass vaccination programs against measles routinely produces a greater drop in mortality than can be attributed just to the decline in measles incidence.
The authors begin by pointing out how successful measles vaccination programs have been; that is, where they have been able to achieve high levels of vaccination. It’s a success that, contrary to what most people realize, goes beyond just preventing measles and causing its incidence to plummet to very low levels in developed countries:
Measles vaccines were introduced 50 years ago and were followed by striking reductions in child morbidity and mortality (1, 2). Measles control is now recognized as one of the most successful public health interventions ever undertaken (3). Despite this, in many countries vaccination targets remain unmet, and measles continues to take hundreds of thousands of lives each year (3). Even where control has been successful, vaccine hesitancy threatens the gains that have been made (1, 4). The introduction of mass measles vaccination has reduced childhood mortality by 30 to 50% in resource-poor countries (5–8) and by up to 90% in the most impoverished populations (9, 10). The observed benefits cannot be explained by the prevention of primary measles virus (MV) infections alone (11, 12), and they remain a central mystery (13).
MV infection is typified by a profound, but generally assumed to be transient, immunosuppression that renders hosts more susceptible to other pathogens (14–17). Thus, contemporaneous reductions in nonmeasles mortality after vaccination are expected. However, reductions in infectious disease mortality after measles vaccination can last throughout the first 5 years of life (5–10), which is much longer than anticipated by transient immunosuppression, which is generally considered to last for weeks to months (16, 17).
They cite a recent report by the World Health Organization (WHO) that examined the nonspecific effect of various vaccines on all-cause mortality (i.e., the effect of the vaccine on causes of mortality other than the disease that it is designed to prevent), which concluded that measles vaccination is associated with large reductions in all-cause childhood mortality, an effect more marked in girls than in boys, but that there is no firm evidence to explain an immunological mechanism for the nonspecific vaccine benefits. To illustrate this, here is a graph from the report summarizing the results:
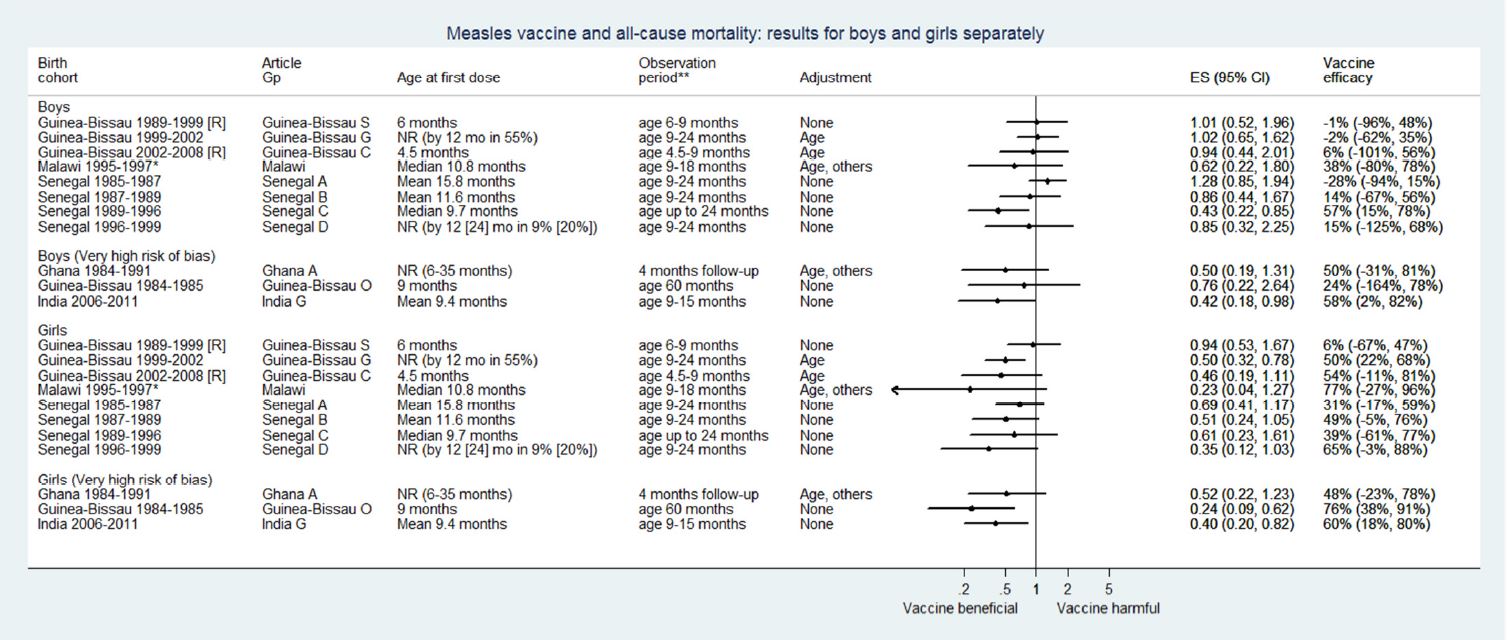
The measles vaccine decreases mortality from causes other than measles more among girls than boys (click to embiggen).
As you can see, most of the studies show a significant decrease in all-cause mortality, an effect that is more marked in girls than in boys. The authors separated studies deemed to be at high risk of bias from those judged to be higher quality, and the effect is still there. Mina et al. note that proposed mechanisms for a nonspecific beneficial effect of measles vaccination include suggestions that the live vaccine might directly stimulate cross-reactive T cell responses or that they might train innate immunity to take on a phenotype like that of immune memory. However, they question whether such effects can explain the long term benefits of measles vaccination and the pre-measles vaccine associations between measles and mortality from other infectious disease. At this point, I can’t help but emphasize that what Mina et al. found is not a new finding that measles vaccination has a robust effect on all-cause mortality, including infectious diseases other than measles. This is a finding that has been observed enough times that it is generally agreed upon. Rather, what Mina et al. did was to test a hypothesis using population-level data that the reason for this effect has to do with modulation of the immune system by the measles virus such that it is less effective in warding off other infectious diseases for a significant period of time after.
So what might explain this effect? The authors invoke a different hypothesis, proposed by Rory D. de Vries at the Department of Viroscience, Erasmus MC, Rotterdam, that a loss of immune memory cells after measles virus infection “resets previously acquired immunity, and vaccination prevents this effect.” The idea is this. Measles often causes depletion of lymphocytes, which rapidly rebound after the disease clears. However, de Vries et al. hypothesize that “massive expansion of MV-specific and bystander lymphocytes masks the fact that pre-existing memory lymphocytes have been depleted” and conclude that “measles virus infection wipes out immunological memory, leaving individuals susceptible to opportunistic infectious agents that would normally be controlled by the immune system.” In a commentary, de Vries argues:
Experimental MV [measles virus] infections in animal models have demonstrated that percentages of infected lymphocyte subsets are higher than previously thought, especially in secondary and tertiary lymphoid tissues [11], [13]. We believe that measles immune suppression mainly results from depletion of immune cell subsets, which is masked by the rapid proliferation of MV-specific and bystander lymphocytes (Fig. 1D). This model is fully compatible with the measles paradox. Clinical studies are required to test our hypothesis that measles immune suppression is mainly a numbers game.
Consider Mina et al. a first attempt at testing this hypothesis at a population level using mathematical modeling of measles cases and mortality from other infections before and after the introduction of widespread measles vaccination campaigns in the US, England and Wales, and Denmark. In fact, the raw data (in Figure 1, if you have access to Science) suggest a very strong correlation between measles infection and death rates from other infections. To provide supportive evidence for the hypothesis, the following had to be true
- Nonmeasles mortality should be correlated with measles incidence data, especially because the onset of vaccination reduces the latter.
- An immune memory loss should present as a strengthening of this association when measles incidence data are transformed to reflect an accumulation of previous measles cases.
- The strength of the association should be greatest when the mean duration over which the cases are accumulated matches the mean duration required to restore immunological memory after measles infection.
- The estimated duration should be consistent both with the available evidence of increased risk of mortality after measles infection compared with uninfected children, and with the time required to build a protective immune repertoire later in life.
Finally, as the authors stated, “To explicitly address whether the observed nonspecific benefits of vaccination can be attributed to the prevention of MV immunomodulation, evidence for the four hypotheses must be present separately within the pre-vaccine eras.” Let’s just say that they were.
For example, when the authors transformed the data as described in #2 and #3, for England and Wales, the best fit occurred centered at a 28 to 28.3-month duration of measles-induced immunomodulation in the pre-vaccine era. In the pre-vaccination era, they obtained an estimated 29.2 month duration for measles-induced immunomodulation in the post-vaccine era. These results were robust and held up to a number of manipulations, including examining various age groups and different disease classes. Looking at the different countries, the authors found strong evidence to support “a generalized prolonged (roughly 2- to 3-year) impact of measles infection on subsequent mortality from other infectious diseases.”
Additional controls only strengthened the authors’ observations. For example, because previous evidence suggests that the immunomodulatory effect of measles virus is stronger in girls, thus leading to a greater nonspecific benefit of measles vaccination, the authors tested whether their model showed this same effect by comparing genders. Using their model, they found “consistently stronger associations among females,” in agreement with existing data, an agreement that held over multiple tests using either the full data set or the pre-vaccine data set. Finally, as an additional control, the authors repeated their analysis, only this time for pertussis, because pertussis is also vaccine-preventable and is not known to be immunosuppressive, like measles. They found no correlation between pertussis incidence and mortality from infectious diseases other than pertussis, and no correlation was observed even when the authors transformed their data in the same way they did the measles data to reflect the sum of previous pertussis cases.
Of course, this study is not perfect. One can always criticize choices made in mathematical models, and the authors do point out a caveat of their study and its strong agreement with previous observations in that other studies have failed to detect long-term immunological sequelae from measles. However, they point out that these cohort studies focused on low-income countries, where high rates of death from opportunistic infections during the acute measles infection tend to drive mortality; in other words, in these countries, so many children die of opportunistic infections and other acute sequelae of measles that effects from long term immunological sequelae are probably masked, given that approximately 50% of all childhood deaths recorded after five years of followup occurred within two months of infection.
The authors end up concluding:
MV infection and vaccination produce strong and durable herd immunity against subsequent epidemics (40). Our results thus suggest an extra dynamical twist: MV infections could also reduce population immunity against other infections in which MV immunomodulation could be envisioned as a measles-induced immune amnesia (17); hence, measles vaccination might also be preserving herd protection against nonmeasles infections.
Measles vaccination is one of the most cost-effective interventions for global health, and our results imply further immunological dividends: mortality (and probably morbidity) reductions linked to measles vaccination might be much greater than previously considered. This is of particular importance today where, especially in wealthy nations, reduced opportunistic infections during acute measles immunosuppression, added to the comparative rarity of infection, has led to a public view of measles as a benign childhood disease. Our findings help dispel the mystery surrounding the disproportionately large reductions in mortality seen after the introduction of measles vaccinations and reinforce the importance of measles vaccination in a global context.
Indeed, it has been noted that, after the introduction of the measles vaccine, not only did measles cases decline in the US, but deaths from infections such as respiratory and diarrheal diseases also fell from 18 per 100,000 before vaccination to 6 per 100,000 after vaccination, or, as the authors state earlier in their study:
Our results show that when measles was common, MV infections could have been implicated in as many as half of all childhood deaths from infectious disease, thus accounting for nearly all of the interannual fluctuations in childhood infectious disease deaths. The reduction of MV infections was the main factor in reducing overall childhood infectious disease mortality after the introduction of vaccination.
Of course, this is just one study and will require replication and studies to expand upon its results, assuming they hold up, but it fits in with other, earlier studies, suggesting that the benefits of vaccinating against measles go beyond preventing just measles. It is also yet another piece of data that puts the lie to claims by the antivaccine movement that measles is not dangerous and that we should believe a silly old sitcom’s view of the measles over the view of pediatricians and scientists, who knew that the measles is not a benign disease but had little to offer with respect to prevention or treatment of the disease other than supportive care. Think of it this way: if measles were such a benign disease and no big deal to worry about, why was such a major effort made to develop a vaccine in the late 1950s and early 1960s? Why was it the next big vaccine after the polio vaccine? This story in the New York Times from 1963 tells the tale:
In terms of frequency, measles is the number one disease of childhood, and it is far from harmless. It renders its victims highly susceptible to other infections. The most dreaded complication is encephalitis, an inflammation of the brain and spinal cord that may lead to permanent damage. In 1958 there were 522 deaths in the United States compared with 255 deaths from polio. In 1960 there were 410 deaths from measles, compared with 260 deaths from polio.
Fifty-two years later, we are now beginning to understand that measles doesn’t just render its victims susceptible to other infections during its acute phase, but that its immunomodulatory effects last as long as three years. Antivaccinationists frequently claim that vaccines “damage” the immune system, despite all the evidence that they do not. Rather, if anything “damages” the immune system, it’s the measles virus, and the protection against that damage is a vaccine.