{kind=link}
While I’m now two full decades out of pharmacy school, I am occasionally invited to return to give a lecture or facilitate a workshop. Pharmacy education has changed a lot since the 1990’s. For me, pharmacy was a Bachelor’s degree program you started right out of high school. Today, students must have a few years of university completed before they can apply (some already have one degree), and the more common degree granted is doctorate-level, the Pharm.D. The clinical training has been bulked up and the practical training is much more rigorous. I see all this as positive change, as the practice of pharmacy has changed along with the education standard. The era of the “count, pour, lick and stick” pharmacist is disappearing as these tasks are automated or delegated to others. Today’s pharmacist has the opportunity to deliver care in different ways, including new roles like vaccine provider, and medication review/drug therapy optimizer. Many find positions that allow them to leverage their drug-related expertise to other areas of the healthcare system.
With pharmacists’ knowledge of drug products it should not be a surprise that they are consulted widely for advice by patients as well as other health professionals. Public surveys on trust show pharmacists lead other health professionals on this measure. It should also not be a surprise that pharmacists can be quite influential in shaping drug use, particularly when it comes to advice about complementary and alternative medicine (CAM), especially when it is used with conventional, science-based drug treatments. After all, drug stores are becoming (to my professional embarrassment) purveyors of all forms of CAM, ranging from homeopathic “treatments” through aisles of herbal remedies, vitamins, and other supplements. One pharmacy I used to work at sold copper bracelets, magnets, salt lamps, ear candles, homeopathic “first aid” kits, and detox packages that were purported to “balance” your pH. If there was a plausibility limit to what this pharmacy would sell, I never saw it reached. I gave the best science-based advice I could, but eventually left due to my concerns about what was on the shelves. But my time in that setting showed me the opportunity to improve care: the pharmacist is well positioned to advise on the evidence for or against any particular treatment, as well as the describe the potential risks with combining CAM with evidence-based treatment approaches.
Given the continued popular interest in CAM, and its proximity to pharmacy practice, research on roles and professional/ethical responsibilities are of interest to academics and researchers. Regrettably, from what I’ve seen in the literature, those with an academic interest or focus in CAM tend to lean towards being believers, rather than scrutinize the promotion of these products and their incorporation into medical therapeutics. (Pharmacy education really needs its own Edzard Ernst, a fierce critic of CAM, who has discussed CAM and health professional ethics). Almost exclusively the criticism of pharmacy and its role as a purveyor of CAM tends to come from outside the profession, with rare, but notable, exceptions.
Mark Crislip has mused that surveys on CAM seem to be an easy path to getting published, given the thousands that exist. Given my personal and professional interests in CAM and pharmacy practice I couldn’t resist reviewing a new survey of attitudes among student pharmacists. Just published in the Journal of the American Pharmacists Association, and entitled Student pharmacists’ attitudes toward complementary and alternative medicine, the paper is from Marwa Noureldin, a pharmacist and graduate student at Purdue University. The survey included 62 questions and was distributed to first, second, and third-year pharmacy students at 10 schools of pharmacy across the United States. There were 887 complete and usable responses. The average student was 25 years old, white, and female. Among the products categorized as CAM, respondents had personally used vitamins (64%), supplements (48%) and massage (39%) in the past.
The survey was divided into three parts – the first section queried attitudes towards CAM, using Likert scales (1=strongly disagree, 5=strongly agree). Questions were adapted from the CAM Health Belief Questionnaire and were modeled after the National Center for Complementary and Alternative Medicine (NCCAM) categorization of CAM:
- Biologically-based therapies (e.g., supplements, vitamins, etc.)
- Manipulative and body-based therapies (e.g., massage, chiropractic & acupuncture)
- “Mind-Body” interventions (hypnosis, biofeedback, prayer)
- “Energy” therapies (e.g., reiki, qi gong)
- Alternative medicine systems (e.g., homeopathy, traditional Chinese medicine, Ayurvedic medicine)
Here’s the results (click to embiggen):
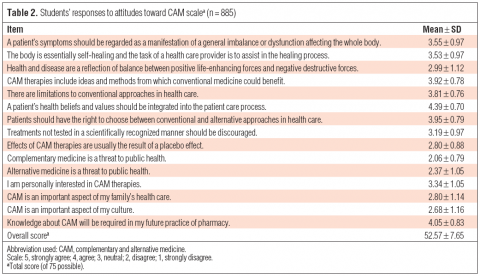
The CAM Health Belief Questionnaire, while it has been “validated” seems to have been designed by CAM proponents as is evident from the common tropes embedded within the survey. Describing health as a consequence of “balance” that is “self-healing” are subtle references to the ideas of vitalism that are common across many alt-med practices. Notably there is no reference anywhere to the fact that CAM therapies are either not proven effective, or are proven to be ineffective. (Any CAM therapy that is therapeutically effective, is by definition not CAM, and should just be called medicine.). The survey paints CAM as a separate set of therapies that represent an equally valid therapeutic choice, rather than more accurately describing it as a collection of therapies and practices that lack evidence of benefit. The surveys also lumps vitamins in as a category of CAM, when some vitamin use can be appropriate and science-based (e.g., folic acid supplementation in pregnancy). It also include interventions like massage, and massage therapy isn’t necessarily CAM at all, depending on the treatment goals.
The student responses lean toward the positive, with most ranging from neutral to strongly agree. This is perhaps not surprising, given how the questions are worded. The strongest support was for the statement “A patient’s health beliefs should be integrated into the patient care process” with 91% of students agreeing. This question is one that could be answered affirmatively by someone that takes a strongly science-based perspective, so what this implies about CAM is unclear. There was also strong agreement that CAM knowledge is required in the practice of pharmacy – a question I also strongly agree with, though my vision for CAM education would likely be quite different than what CAM proponents would like to see. As I have argued before, specialized CAM training in academia is designed and delivered to distract from the fact that CAM (often branded as “integrative medicine”) attempts to embed a double standard of evidence for products and procedures that don’t meet the standard of care for medicine. It should not be surprising then, that students who had taken previous CAM courses had much more favorable views towards the statements in the survey than students without any formal CAM coursework (55.89 vs 48.87, respectively).
The second part of the survey asked about views on acceptability of using CAM with “conventional medical therapies” (the authors’ words), again using the same Likert scale:
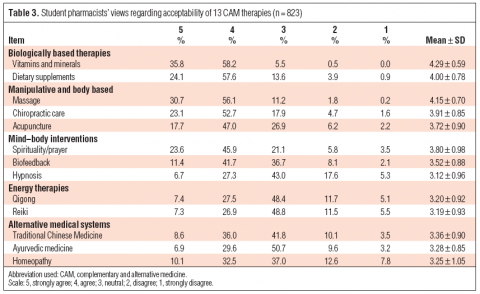
Few students disagreed with any CAM therapy. There was the greatest support for vitamins and minerals (94%, mean 4.29) which could include the science-based use these products. But there was strong support for demonstrably ineffective treatments like acupuncture, with 64% agreeing it was acceptable. Even homeopathy, which any pharmacy student with basic medicinal chemistry skills ought to know is absurd, was supported by over 40% of students. In fairness, these questions could be interpreted in different ways – I agree there are no medical or therapeutic reasons why homeopathy cannot be taken concurrently with actual medicine. However, I’d say the same about qi gong and reiki, yet students gave somewhat less support to concurrent use of those treatments.
Finally, students were asked for the influences on their own philosophy about CAM:
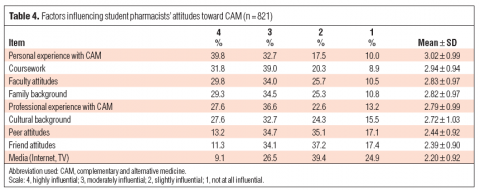
The biggest influence was personal experience (“It worked for me”?), which exceeded coursework, faculty attitudes, family and professional experience. Surprisingly there was no explicit question about the direct influence of the scientific evidence itself. Perhaps disappointingly for bloggers like myself, media (including the internet) was cited as the least popular influence, with 25% indicating it was “not at all influential”.
The discussion section of the paper raises more questions about the overall intent of the survey. Negative opinions about CAM (such as concerns about safety and efficacy) seem to be viewed as problems that can be addressed with more CAM education, rather than crucial issues that call into question the entire endeavor of CAM as a distinct system of treatment. Completely absent from the discussion is any statement about the double standard created by specialized CAM education – the authors draw conclusions that seem to suggest that mixed or negative opinions on CAM are problematic, and that more CAM education is advantageous for pharmacy practice.
The limitations to surveys like this are substantial, which needs to be considered as we study the findings. Given this was a voluntary survey, with a low response rate (23%), it’s quite likely that non-responder bias is a factor. It is plausible that those that are indifferent to CAM, or have critical perspectives, may not have participated in the survey. A second factor was the exclusion of fourth (final) year students from the survey. It’s conceivable that students in their final year might have more critical perspectives on CAM. A third limitation is the use of NCCAM’s categorization of CAM which incorporates science-based therapies alongside rank quackery. The result is a mix of science and pseudoscience, bundled up as “CAM”, which could increase positive perceptions, giving unscientific and disproven treatments the appearance of being deemed acceptable. Finally, the statements and questions were worded in ways that fail to distinguish between what’s appropriate from a science-based perspective, and what’s acceptable from a patient-focused perspective. I would never recommend homeopathy to a patient and would actively advise against its use. However, to an insistent patient, I would assure them that concurrent homeopathy use poses no medical consequences. The survey fails to distinguish between the two scenarios.
Conclusion
This survey on CAM attitudes paints a concerning portrait of American pharmacy students. However, limitations in the survey process may have created biases that could have exaggerated the overall perspective presented. More concerning than the results themselves are the researchers’ interpretation of this data: Critical and negative perspectives on CAM seem to be viewed as problematic, rather than positive examples of good critical thinking.
One lesson from surveys like these is they illustrate the educational goals of CAM proponents. Just like “integrative” medicine that is making its ways into academic hospital settings, CAM education on campus is another tactic that is being used by proponents to shape health professional attitudes and perspectives early in their careers. The objective is obvious: normalize pseudoscience with students, and watch it become embedded into pharmacy practice.
Is this going to change? Unless there is a deliberate and explicit attempt to call out and push back against the degradation of academic and scientific standards created by existing forms of CAM education and “integrative medicine” programs, we should expect to see a growing normalizing of pseudoscience in health professions like pharmacy.
Reference
Noureldin M. Student pharmacists’ attitudes toward complementary and alternative medicine, Journal of the American Pharmacists Association, e205. DOI: 10.1331/JAPhA.2013.12212