{kind=link}

Does ibuprofen really raise your risk of heart failure by 83%? No.
Do you ever take ibuprofen? Naproxen? Cold medication with an anti-inflammatory ingredient? The non-steroidal anti-inflammatory drugs (NSAIDs) are among our most well-loved medications. We start giving them in infancy, for fever, and continue use through to adulthood for everyday aches and pains. But it’s our later stages of life when we really ramp up the use, and daily consumption becomes common for conditions like arthritis. While they may be easily accessible and included as ingredients in thousands of consumer products, NSAIDs have a long list of potentially serious side effects. Not only can they cause stomach ulcers and bleeding by damaging the lining of the gastrointestinal tract, they can also increase the risk of fatal cardiovascular disease. Now there’s new research that looks at the relationship between NSAIDs and heart failure, a condition where the heart cannot pump adequately and appropriately. The study, “Non-steroidal anti-inflammatory drugs and risk of heart failure in four European countries: nested case-control study” resulted in some fairly dramatic, alarming headlines:
Headlines like this suggest that NSAIDs are killing us indiscriminately, which may make you wonder how so many of us manage to have lived this long. And while The Daily Mirror got the facts wrong, they quoted from a well-conducted study. There is a real risk of heart failure from NSAIDs. But context is everything.
From natural origins, dozens of drugs
All NSAIDs act in a similar manner, interrupting the production of inflammatory and pain-related hormones called prostaglandins. Since the introduction of acetylsalicylic acid (ASA or Aspirin) in 1897, more than two dozen chemically-related drugs have been developed. And while your individual results may vary with each NSAID, research shows there isn’t much of a difference overall in how effective they are. However, the risks and side effect profiles of the different NSAIDs can differ, in some cases significantly. Most of us are familiar with the gastrointestinal side effects, which led to the development of the “COX-2” NSAIDs, intended to reduce those effects. The cardiovascular risks of NSAIDs were poorly understood until the worldwide withdrawal of the COX-2 Vioxx (rofecoxib), which triggered multiple studies of the cardiovascular risks of all of the NSAIDs. Multiple confirmatory studies have now clearly established that most NSAIDs (except ASA in low doses) are associated with an increased risk of cardiovascular events, like heart attacks. And over time, further studies have been done to identify if NSAIDs cause other negative effects. Which brings us to this paper.
Do all NSAIDs cause heart failure?
The relationship between NSAIDs and heart failure has already been identified in other studies. NSAIDs can more than double your underlying risk of heart failure. But in most of us, our underlying risk of heart failure is low, so the increased risk is trivial and largely irrelevant. Sensibly, current treatment guidelines recommend caution in those at risk of heart failure, and avoidance of NSAIDs in those with confirmed heart failure. The relative risk of the different NSAIDs is less well understood, so this study examined the type of NSAID used, and the dose.
This new study was a large, sophisticated analysis of NSAID users in five countries. It was a case-control study that identified those who had been prescribed an NSAID (note: not casual users) and then looked to see if they were subsequently admitted to a hospital for heart failure. The rates of hospital admission for heart failure were compared to up to 100 other controls, who didn’t take an NSAID, but otherwise were matched (e.g., same age/sex) to the NSAID users.
The analysis described is quite complex given the multiple datasets and limitations of each. The analysis looked at each NSAID, as well as the prescribed daily dose.
The findings
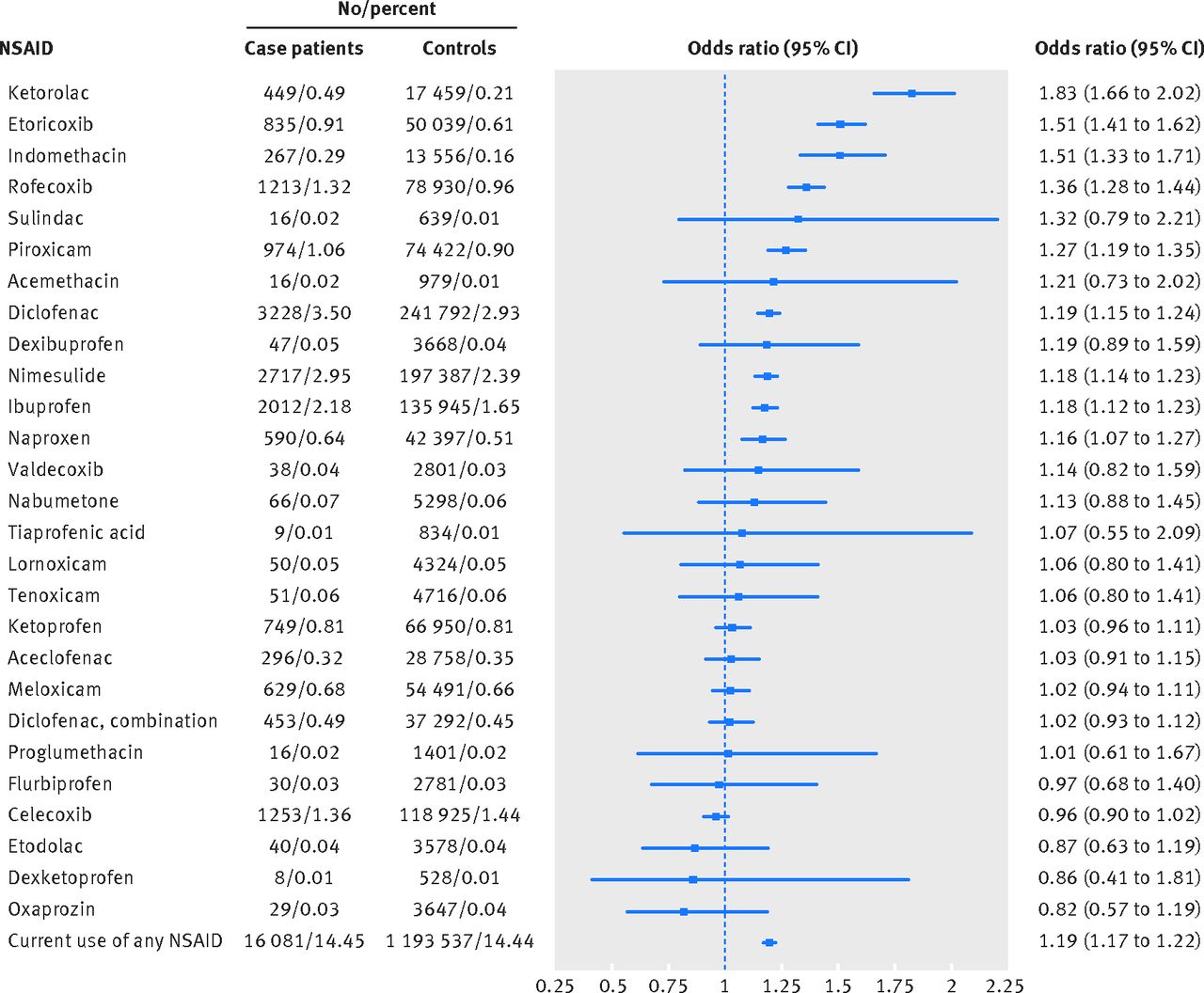
The study found over 16,000 cases and matched them to 1.2 million controls. The average age of was 77 in the treatment group and 76 among controls, with about 45% men. The bottom line from this study is that all NSAIDs are not the same. The degree of risk seems to vary quite significantly. In this diagram, anything that straddles the line is statistically non-significant. Any drug that is over to the right is associated with a statistically significant increase in heart failure. The rarely-used NSAID ketorolac almost doubles the heart failure risk (which is what The Daily Mirror quoted), while ibuprofen is associated with less risk: a 20% relative risk increase. And surprisingly, Ketorolac, etoricoxib, and indomethacin all cause more heart failure than the withdrawn rofecoxib (Vioxx). Interestingly, celecoxib (Celebrex) doesn’t appear to raise the risk of heart failure at all.
Click to embiggen
The composite (overall) result in in the bottom line, showing that current users of any NSAID have a 20% higher risk of heart failure than past users.
What does this mean to me?
This new evidence gives more support and context to our understanding of how NSAIDs can harm. NSAIDs do raise your risk of heart failure, although some are worse than others. However, if your underlying risk of heart failure is low, then occasional NSAID use is not a concern. As your risk of heart failure increases, your risk of experiencing harm from an NSAID increases, too. So do the risks outweigh the benefits? Ultimately this comes down to your individual factors: your reasons for use, any risk factors for disease you may already have, and the expected benefits. When used on a short-term basis by those who are not at risk of heart failure, the potential harms are slight. So don’t use NSAIDs indiscriminately, but don’t panic, either.
Photo from flickr user Mike Mozart used under a CC licence.