
{kind=link}

Would it be ethical to conduct a clinical trial where you could be randomly assigned to drink coffee, or to abstain from it? Notwithstanding any of your personal feelings about the beverage, it would be ethically appropriate to verify that, at minimum, coffee consumption wasn’t harmful. Given coffee’s massive, world-wide popularity, its safety may seem self-evident. Yet it’s not impossible that coffee could be causing subtle health effects (say, very slight increases or decreases in the risk of common diseases, like cancer or cardiovascular disease) that would be undetectable without some sort of population-level study. Observational studies have shown mixed effects of coffee consumption on a range of health conditions, including pregnancy outcomes. But what are the overall effects? That’s what a new study set out to understand.
What are the chemicals in coffee?
Coffee was possibly the original “functional food”, in that it was routinely consumed for specific effects. Coffee starts as the unroasted green been (of Dr. Oz infamy) and through roasting, undergoes chemical changes to produce over 1,000 biologically active compounds. The ingredient that most people associate with coffee is caffeine, thought to be produced by the plant as an insecticide. But there are many other ingredients that have potential medicinal effects, including chemicals identified to have anti-oxidant, anti-inflammatory, anti-fibrotic, and even anti-cancer properties. The extent of roasting, and the brewing method will influence what ends up in your cup. Interestingly, genetic differences and even the microbiome in your digestive tract will ultimately affect which components are ultimately absorbed into the bloodstream. Recognizing all of these potential variations, only population-level studies can be expected to give us meaningful data.
What was the objective of this study?
Given the popularity of coffee there has been considerable research between consumption and different health outcomes, including mortality, cancer, cardiovascular disease, as well as effects in pregnancy. Almost all research has been observational in nature, in that there was no randomization – meaning causality couldn’t be inferred. One of the more interesting areas of study has been the relationship between coffee consumption and liver disease, including liver cancer, where there appears to be signals of a substantial benefit. Before randomizing patients to drink (or not drink) coffee, a comprehensive analysis of health effects was felt to be warranted. If there were signs of possible harm, randomizing people to drink coffee would not ethical. So this study sought to summarize all of the available evidence of coffee consumption and health outcomes.
This new study by Robin Poole and colleagues is entitled “Coffee consumption and health: umbrella review of meta-analyses of multiple health outcomes.” It was published in the BMJ earlier this month. This was an umbrella review, which is a summary of existing systematic reviews and meta-analyses. The authors sought to evaluate all evidence for associations between coffee consumption and multiple health outcomes. This was specifically a study of coffee, not of caffeine alone, recognizing that the health effects of coffee could be based on any of (or a combination of) the chemical constituents. A comprehensive search of the medical literature found 201 meta-analyses in 135 articles studying 67 different endpoints. There were also 17 meta-analyses found of randomized controlled trials in six articles with 9 outcomes. Here are the compiled results for (a) High versus low coffee consumption (b) Any versus no coffee consumption and (c) Consumption of “one extra cup per day”. Each figure shows relative risk estimates for the ten most harmful associations, and the ten most beneficial associations.
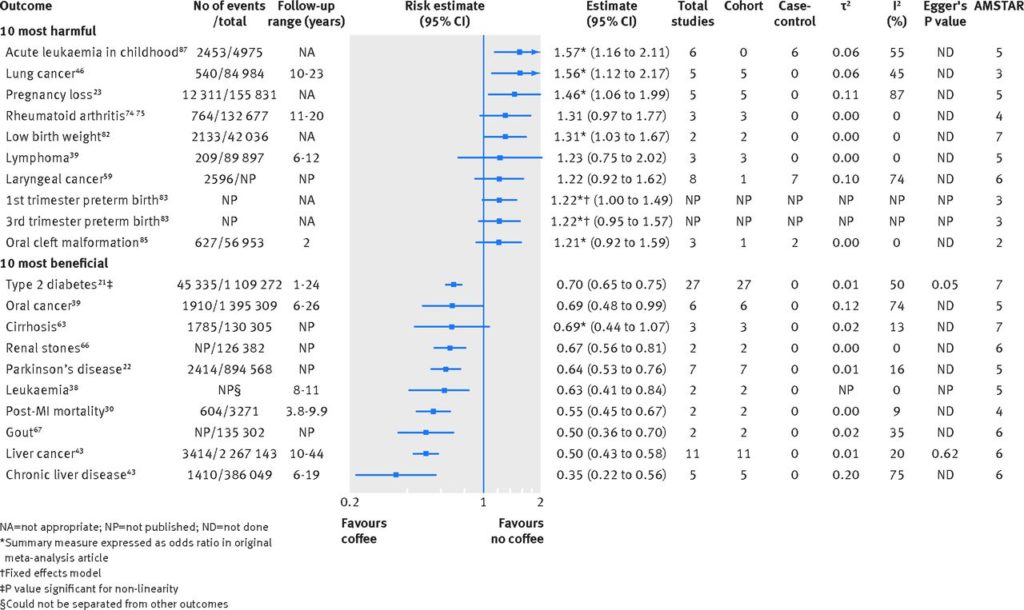
High versus low coffee consumption and associations with multiple health outcomes. Estimates are relative (not absolute) risks.
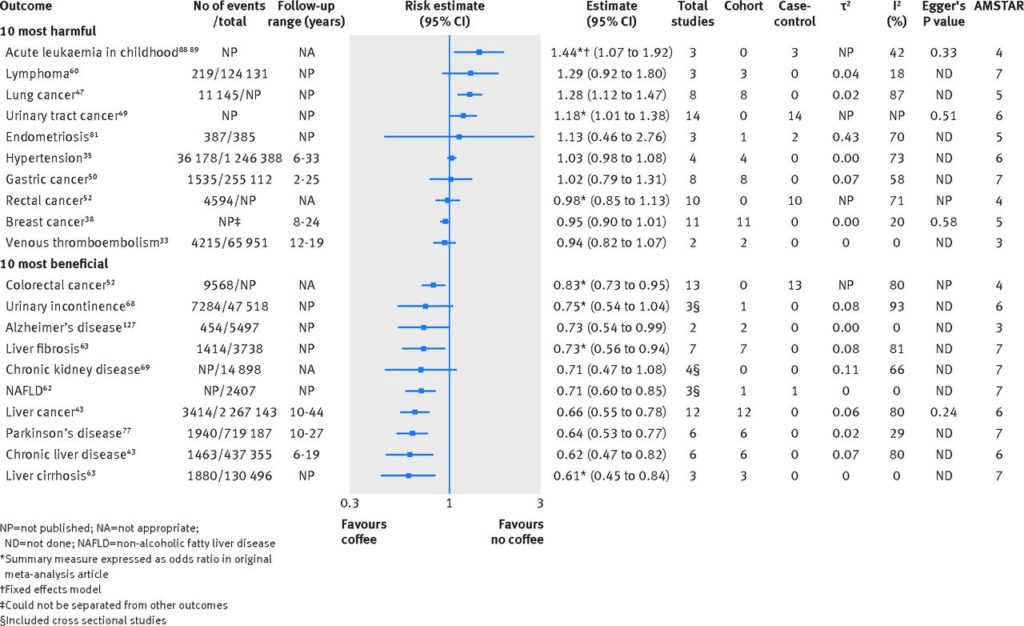
Any versus no coffee consumption and associations with multiple health outcomes. Estimates are relative (not absolute) risks.
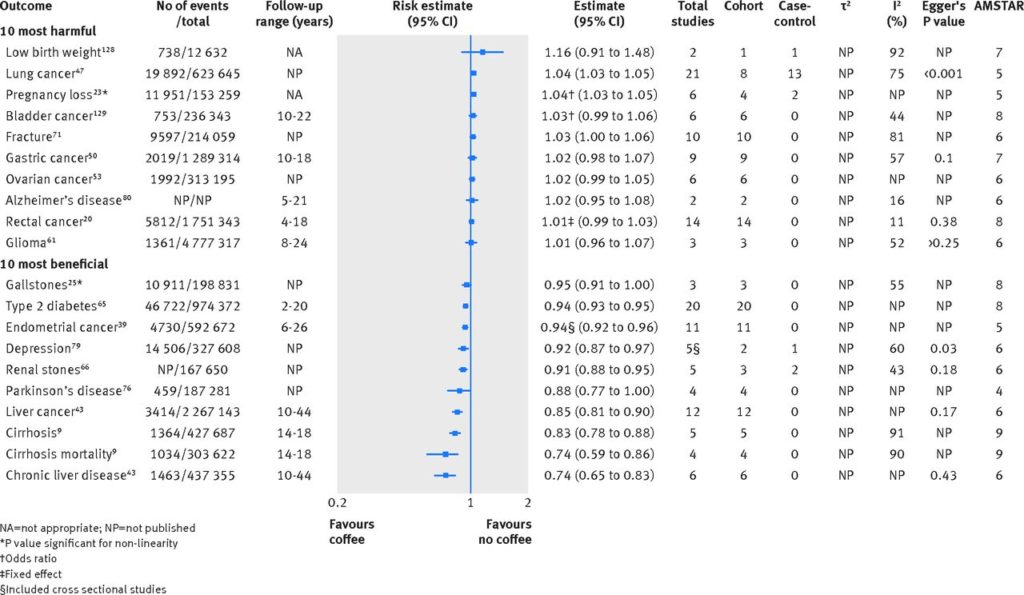
Consumption of one extra cup of coffee per day and associations with multiple health outcomes. Estimates are relative (not absolute) risks.
As you can see, the associations for liver disease, including liver cancer, appear the most beneficial. It’s worth reiterating that given the associations are from observational studies, they cannot prove cause and effect. It’s also worth noting that the effects are reported as relative risks, not absolute. And overall, those relative effects are small.
In terms of all-cause mortality, the authors noted a recent meta-analysis by Grosso concluded that the largest benefit was observed in those drinking 3 cups of coffee per day, giving a relative risk of 0.83 compared with no coffee consumption. The same study found that this effect held for cardiovascular disease (including heart attack and stroke) as well. Compared with non-drinkers, risk were reduced by 19%. More coffee was not harmful, but the benefit was less pronounced, and became insignificant at the highest intakes. This is despite what have been observed to be unfavourable effects on blood lipid levels themselves. Interestingly, coffee consumption had marginally beneficial effects on blood pressure.
In terms of cancer, a lower overall incidence of cancer was found in high versus low consumption of coffee, but the effects were modest. There was a harmful association found between coffee and lung cancer (high versus low consumption) but the effect was reduced when smoking was adjusted for, with no association found in never smokers.
In addition to the beneficial effects observed in liver cancer, coffee consumption was observed to reduce risk of a number of liver diseases, including non-alcoholic fatty liver disease (29% lower risk, any versus no consumption), liver fibrosis (27% lower risk), and liver cirrhosis (39% lower risk).
In terms of effects in pregnancy, there are consistent signals that coffee may be harmful. High versus low consumption is associated with a greater risk of low birth weight, pregnancy loss, and first and second preterm birth. No effects were observed in third trimester preterm birth, neural tube defects, and congenital malformations. Interestingly there’s also consistency in the associations between coffee consumption in pregnancy and childhood leukemia, which is illustrated in the two tables above.
Coffee for everyone?
There are countless reasons why coffee drinkers could differ from non-drinkers. What we can conclude from this umbrella review is that coffee consumption is usually safe, and that there is the suggestion that regular consumption may actually be beneficial. With the exception of consumption during pregnancy, there is also reassuring evidence that coffee intake is unlikely to cause harm. So if you don’t drink coffee, should you start? If you don’t like the taste of coffee, the beneficial effects are modest enough that you’re likely not giving up a remarkable benefit. But if you do enjoy your coffee, and want to maximize the possibility of health benefits, keep you consumption moderate (around 3 cups per day). And feel satisfied that you’re possibly doing something that’s good for you.
Photos via flickr users dazegg and Lindsey Turner used under a CC licence.
Full disclosure: I drink coffee, usually 2 cups per day.