{kind=link}
[Editor’s note: This is a guest post from two contributors, Drs. Kenneth R. Foster and Chung-Kwang Chou, exploring the controversy of “Havana syndrome“. Welcome!]
“An individual assigned to the U.S. Embassy in Cuba was awakened one night at home in Havana by severe pain and a sensation of intense pressure in the face, a loud piercing sound in one ear with directional features, and acute disequilibrium and nausea”, began a 2020 report by the National Academies of Sciences, Engineering and Medicine (NASEM) that investigated the problem.
The first incident occurred in November 2016. In early February 2017, a second person reported an unexplained onset of similar symptoms. The Embassy alerted its employees as a group that they could be under attack and requested any employees to report similar symptoms. Ultimately 68 US Embassy employees in Havana reported symptoms. The incidents occurred in residences or hotel rooms, not in the Embassy itself.
According to a heavily redacted June 2018 report by the U.S. Department of State (DoS), the Embassy had a series of “town hall” meetings with Embassy staff. On February 6, 2017 the embassy medically evacuated the first patient and, the end of September 2017, the Secretary of State ordered the departure of all non-emergency staff in response to what the DoS report termed the “health attacks”. The CIA withdrew its personnel from Havana as well. The embassy installed “recording devices that are geared to record high-frequency sounds” in some residences, without finding the source of the problem. “As of [June 2018], the who, what, when and sometimes the where behind these incidents is still unknown”, the report concluded.
As of mid-2018, according to the DoS report, “24 Embassy Havana community members have been medically confirmed to have sustained brain injuries while serving in Havana with the severity of injury ranging from mild impairment to injuries in a few patients so severe they may never be able to return to their previous jobs”. Other US employees at the U.S. Consulate in Guangzhou, China described similar experiences. At least 14 employees of the Canadian Embassy in Havana also reported symptoms. A February 2021 news report describes a similar experience to a covert CIA agent while he was sleeping in a Moscow hotel room. After suffering for months with crippling headaches, the agent retired prematurely from the Agency.
The symptoms typically occurred in two stages: some (not all) of affected individuals perceived loud noises accompanied by a headache, and a feeling of pressure in the head. A few days later they experienced vestibular disturbances (balance difficulties) and cognitive deficits (“brain fog”).
An account, relayed to us by a member of the NASEM panel that investigated the matter, described a “funny clicking sound and the feeling of being pushed or pressure with head pain”. These sensations persisted while the individuals were “outside or in front of a window, and they went away when they went behind a wall or left the room”. Multiple individuals, who had worked in Havana and Guangzhou who were interviewed by members of the NASEM panel, gave similar accounts, emphasizing the directionality of the pressure and its attenuation behind walls.
Medical follow-up
The DoS partially evacuated the Embassy in Havana. Affected individuals were referred to U.S. doctors for treatment and evaluation. Some went to an otolaryngology (ear specialist) group led by Michael Hoffer at the University of Miami (UM). Hoffer, a former military physician who had done extensive research on traumatic brain injury, conducted a series of vestibular (inner ear and balance) tests on the patients. Other individuals, including some of patients who had previously been evaluated at UM, were evaluated by a head injury group led by Doug Smith at the University of Pennsylvania (Penn; note that Dr. Foster is an Emeritus Professor at Penn but had no connection with this work).
The UM group reported that all 25 individuals it examined had vestibular (inner-ear) damage and suggested that their findings were reminiscent of mild traumatic brain injury (mTBI). Using a different set of tests, the Penn group concluded that the individuals “appeared to have sustained injury to widespread brain networks”, a different diagnosis but likewise pointing to mild brain injury. Hoffer concluded:
It does not seem imprudent to speculate that a highly specific unidentified energy exposure, perceived as a sound or pressure, could be producing an inner ear disturbance or demonstrate findings suggestive of an mTBI.
Both studies were challenged for a variety of reasons that can be roughly summarized as over-interpreting weak and in most respects normal clinical findings. The Penn findings, in particular, were challenged in a scathing editorial in the journal Cortex, and a devastating review by Neuroskeptic.
Late in 2017 at the request of the DoS, the U.S. Centers for Disease Control and Prevention (CDC) reviewed medical records of 95 individuals reporting symptoms, including those receiving care at UM and Penn as well as patients seen by DoS medical facilities. The records varied greatly in completeness, many even lacked information about when the symptoms began, and dates of arrival and departure from Cuba. More than a third lacked rudimentary information such as dates of birth and gender of the individuals. The CDC study had no comparison group to allow it to assess risks and mitigation factors for the symptoms and no independent way to diagnose the health problems. It could only line up symptoms in secondhand medical data in search of patterns.
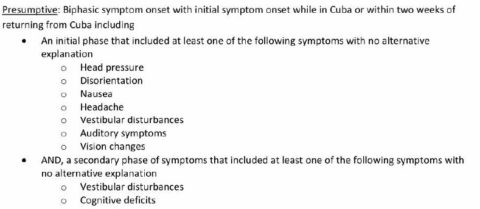
Table 1. Definition of “presumptive” cases in CDC report.
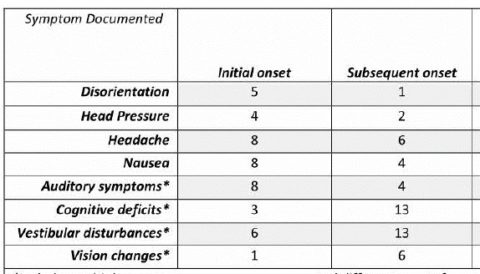
Table 2. Symptoms reported by 15 presumptive cases, in initial stages (initial onset) and later stages (subsequent onset) of symptoms. The individuals reported multiple symptoms so totals in each column added to more than 15.
The CDC identified 15 “presumptive” cases based on similarities of the patients’ symptoms. These cases had a “biphasic” onset of symptoms, with some symptoms developing immediately after their presumed exposure, followed a few days or weeks later by other symptoms (Table 1). The most commonly reported “initial onset” symptoms were headache, nausea, and auditory symptoms, and the most commonly mentioned “subsequent onset” symptoms were cognitive deficits and vestibular disturbances (Table 2). All of the symptoms were self-reported and nonspecific, so they could have had other causes.
Responding to their employees’ concerns, in 2019 the DoS turned to the National Academies of Sciences, Engineering and Medicine (NASEM) which put together a blue-ribbon panel of distinguished physicians, engineers, and scientists to investigate. The panel was charged to “review the cases, their clinical features and management, epidemiologic investigations, and scientific evidence in support of possible causes, and advise on approaches for the investigation of potential future cases”.
However, the panel worked under constraints that limited its ability to carry out these charges. The panel had no access to patient records or results obtained by previous investigators, lacked access to classified information, was not permitted to contact Cuban physicians who were likewise mystified by the events, and – until late in its work – could not even read the CDC report. It did, however, interview some of the affected individuals who had worked at the US Embassy/Consulate in Havana and Guangzhou. The panelists, which included very senior neurologists, neuro-otologists, and psychiatrists, did not consider the symptoms typical of any known psychiatric disorder.
The panel met three times, in December 2019, February 2020, and May 2020. In its first meeting, it heard from Hoffer and Smith – but not from scientists who had criticized their studies. In its second meeting, the panel heard from three speakers who had studied the biological effects of radiofrequency (RF) energy or microwaves (part of the RF spectrum that is used by communications and other applications). Two of these speakers had previously proposed that pulsed microwaves were the cause of the problems. Three additional speakers were affiliated with the Air Force Research Laboratory (AFRL), which had developed a high-powered pulsed microwave weapon (THOR) to destroy drones; little information is publicly available about that weapon, and is presumably classified.
Thus, the panel was steered by its agenda to focus on microwave weapons as the cause of the symptoms. The panel lacked the time and resources to explore other theories. In particular, it lacked participation by a social psychologist with expertise in mass psychogenic illness (an explanation proposed by, among others, the famous psychiatrist Simon Wessely of King’s College London).
In its final report (June 2020) the NASEM panel concluded that the symptoms were “consistent with a directed radio frequency (RF) energy attack”. Six months later, after a prolonged review by the government, the report found its way to the media, leading to numerous reports about “directed microwave weapons” possibly being used against the embassy employees.
Microwaves on the brain
Two main theories, not necessary mutually exclusive, have surfaced to explain what has come to be called the Havana syndrome. The first was that the employees were targeted by a weapon – the NASEM panel thought that the evidence pointed to microwave energy as the cause of the symptoms.
“Microwaves” entered the conversation initially through an almost comical series of non sequiturs: The employees heard unexplained sounds. In its investigation, the FBI found no evidence that an attack using acoustic weapon had occurred. Under some specialized exposure conditions, pulsed microwaves can elicit auditory sensations in some individuals. Ergo, microwaves were the cause of the problem.
This theory rests on the so-called microwave auditory effect (sometimes called the Frey effect), which two of the present authors studied in the early 1970s (KRF and C-KC). When a pulse of RF energy is absorbed in a person’ head, the resulting temperature rise causes tissue to expand slightly. This launches a pressure wave that propagates throughout the head to the cochleae, eliciting auditory sensations. Under realistic exposure conditions, the temperature rise is very tiny (microdegrees), and the pressure wave is far too weak to cause tissue injury.
This explanation accords poorly with the experiences reported by the embassy staff. Some (but not all) of the subjects perceived loud sounds from a particular direction, whereas the auditory sensations from pulsed microwaves are threshold hearing phenomena that requires the subject to be in a quiet room to perceive. The pressure waves are generated within the head and the sensations are not externally localized.
In the 1970s, the microwave auditory effect was chiefly studied using radar pulses. Recently, directed energy weapons such as THOR transmit extremely intense microwave pulses that would induce stronger but much briefer pressure waves in the head than old-style radar pulses. However, limited studies show that the microwave pulses transmitted by such a weapon are unlikely to cause tissue damage. Moreover, the equipment is large. It is hard to see how one could navigate such equipment to provide a line-of-sight view to a window in the victim’s home or hotel in what U.S. Senator Rubio called “the most heavily monitored city in the most heavily monitored country in the Western Hemisphere“.
The panel bolstered its conclusion by citing a number of RF bioeffects studies. These included speculative theories that have never been accepted by health agencies or expert groups but are sometimes invoked by activists to justify their concerns about health hazards of cell phones and Wi-Fi. The report also pointed to the long history of microwave bioeffects research in the former USSR, which reported many biological effects but typically failed to meet present standards of scientific quality. It did not cite the many extensive reviews by Western health agencies and expert groups that failed to uncover clear evidence for hazards at exposure levels below international exposure limits. Now, after seven decades of controversy, the recognized injuries from acute overexposure to microwaves only involve excessive heating of tissue.
In short, the microwave weapon theory falls apart on even cursory examination, being neither consistent with the facts of the case, nor supported by a plausible biophysical argument, nor supported by any observations of microwaves at places where the presumed exposures took place.
Other physical agents have been reported to cause effects reminiscent of those reported by the employees. High intensity infrasound (which has a frequency below 20 Hz, the threshold for human hearing) has been reported to cause dizziness, vertigo, imbalance, nausea, and other effects – similar to symptoms reported by the Embassy staff. According to French journalist Juliette Volcler in Extremely Loud: Sound as a Weapon, the U.S., U.K., Russia, and other countries have at some time or other launched programs to develop nonlethal infrasound weapons, leading to occasional stories of uncertain reliability in the press. However, a 2007 review by two researchers in a U.S. directed energy bioeffects laboratory concluded that infrasound weapons are not feasible as military weapons, in part because of the difficulty of generating and transmitting infrasound waves at militarily useful amplitudes.
But such weapons exist! In September 2019, Steven King, a tech reporter specializing in China, reported that China “had created the world’s first portable sonic gun for riot control”. The developer, Xiujuan Xie (Technical Institute of Physics and Chemistry, Beijing) had earlier (2011) developed a novel generator to produce high intensity sound waves. The device that she described operated at a frequency (71 Hz) that is above the infrasound range but its design could undoubtedly be adapted to generate high intensity infrasound as well.
No technical information about the sonic gun is available. According to news reports, the device causes “extreme discomfort, with vibrations in the eardrums, eyeballs, stomach, liver and brain”. At some level of exposure, such effects would clearly be dangerous, although brief exposures at modest levels might be very unpleasant to an individual but not cause lasting damage. Since, as King reported, the “project team has completed its assessment of the device’s effects on the body” it presumably has good data on its effects on humans. Or maybe not.
But the story is not completely consistent. The weapon, shown in King’s article, resembles a rifle – and seems implausibly small for something that operates on gas at very high pressures and temperatures and consumes hundreds of watts of power as described in Xie’s original reports.
It’s in your mind
A completely different theory, in many respects more plausible, proposes that the symptoms were a manifestation of a mass psychogenic illness. This illness, formerly called mass hysteria, refers to “outbreaks of illness attributed to a toxic agent but for which no plausible organic cause is found“.
Writing from the perspective of social psychiatry, Bartholomew and Baloh proposed that the “Havana syndrome” was a mass psychogenic illness (MPI). They write:
…symptoms such as difficulty concentrating, brain fog, memory problems, and sleep-related complaints (e.g., drowsiness, insomnia) were present in nearly all patients, but are also common in those with anxiety, depression and both individual and epidemic forms of psychogenic illness.
Bartholomew and Baloh noted that the diagnoses of brain injury by the UM and Penn groups are hardly unambiguous. Physicians can “shape the presentation of symptoms through suggestion, as many of these complaints are common in the general population”. “The process of referring patients with non-specific symptoms to a clinic specializing in brain trauma can shape the symptoms into a specific pattern”.
In other words, the medical advice that a patient gets can depend on the kind of specialist he or she visits. This effect is well known to ordinary consumers: if my car makes a funny noise and I take it to a transmission shop for repair, the diagnosis is likely to have something to do with the transmission. That, roughly speaking, is analogous to what the DoS did with their employees who complained about symptoms.
In their 2002 article “Protean nature of mass sociogenic illness“, Bartholomew and Wessely gave historical examples of MPI. In the 1930s and 1940s, for example, a series of “mad gasser” attacks were reported in American towns, when residents became agitated by unfamiliar smells and assumed that they were the result of a gas attack. In Mattoon IL, more than two dozen cases were reported in 1944 of gassings by an unknown assailant, producing symptoms including “breathlessness, nausea, headache, dizziness and weakness”. No physical evidence or suspect were ever found, and the presumed victims recovered quickly. (By contrast, some of the affected individuals in Havana reported lasting disabilities).
The feeling is inescapable that something had happened to the employees who had experienced unusual and disquieting sensations while standing in front of their doorways. But those were only a small fraction of the Embassy employees who reported symptoms. According to Alon Friedman (professor of neuroscience at Dalhousie University, Halifax) who investigated the Canadian cases, only one of the affected Canadians had reported auditory sensations and acute events.
The NASEM panel “considered [the possibility of a mass psychogenic illness], while keeping in mind that the likelihood of mass psychogenic illness as an explanation for patients’ symptoms had to be established from sufficient evidence. It could not be inferred merely by the absence of other causal mechanisms or the lack of definitive structural injuries.” (The panel did just that in pointing to microwave attacks). Bartholomew, Wessely, and other social psychologists who have studied many incidents of MPI could have provided an expert assessment of this case as well, had they been asked.
After reviewing all publicly available evidence on the issue, we honestly have no idea what had happened. Mitchell Valdés-Sosa, director of the Cuban Neuroscience Center in Havana who is leading Cuban efforts to investigate the matter, emphatically pointed out to one of us that the Cuban government had no interest in harassing US diplomats given the urgent need to roll back the US economic sanctions which have devastated the Cuban economy.
However, in the murky world of intelligence, other calculus might apply. According to an October 2020 report in The New York Times, some of the affected individuals in China were CIA agents meeting with counterparts in other countries to discuss ways to counter Russian covert operations. According to the Times report, some members of the US intelligence community believed that Russia was to blame for the attacks in China. We will likely never know.
The window of opportunity for resolving this series of incidents has passed. The US response was simply too slow and uncoordinated. “Despite some early attempts to provide consistent support for potentially affected employees”, the 2018 DoS report concluded, the DoS response was hampered by the “lengthy vacancies at the Under Secretary level” with “no senior official [being] identified as having ownership of the issue”. The report found the “delay of almost six weeks between first knowledge of injury and the first briefing of Embassy staff to be unfortunate and the exclusion of family members from this knowledge to be unjustified, given the incidents were taking place at residences”. It appears that slowness of the Trump administration in filling senior DoS positions directly contributed to the unacceptably slow response of the DoS.
Science based medicine broadly refers to medical evaluation and treatment supported by the best available evidence. That project is complicated for the Havana patients by the many nonmedical factors surrounding the case, which may involve possible spy vs. spy machinations, classified information about weapons systems, and the policies of the Trump administration towards Cuba, China, and Russia that undoubtedly affected the responses of the DoS.
From the extensive redactions in the DoS report (which include, for example, almost the entire timeline of the events), it seems that the government knows a lot more about the affair than it has disclosed. The best one can hope for is that the government is better prepared to respond properly the next time a similar thing happens. If a weapon were involved (we are not convinced that one was) it surely will.
 Dr. Kenneth R. Foster received the Ph.D. degree in physics from Indiana University, Bloomington, IN, USA, in 1971. He was with the U.S. Navy, Naval Medical Research Institute, Bethesda, MD, USA, from 1971 to 1976. Since 1976, he has been with the Department of Bioengineering, University of Pennsylvania, Philadelphia, PA, USA, where he is currently Professor Emeritus. He has been involved in studies on the interaction of nonionizing radiation and biological systems, including mechanisms of interaction and biomedical applications of radio frequency and microwave energy. In addition, he has written widely about scientific issues related to possible health effects of electromagnetic fields. He has authored approximately 170 technical papers in peer-reviewed journals, numerous other articles, and two books related to technological risk and the law. In 2016 he received the d’Arsonval Award from the Bioelectromagnetics Society for contributions to the field of bioelectromagnetics. He is a longtime member of TC 95 of the IEEE International Committee on Electromagnetic Safety (which sets safety limits for radiofrequency energy) and a member of the Physical Agents Committee of the American Conference of Industrial Hygienists, among many other professional activities. He is Life Fellow of the IEEE, and fellow of the American Institute for Medical and Biological Engineering and the Electromagnetic Academy.
Dr. Kenneth R. Foster received the Ph.D. degree in physics from Indiana University, Bloomington, IN, USA, in 1971. He was with the U.S. Navy, Naval Medical Research Institute, Bethesda, MD, USA, from 1971 to 1976. Since 1976, he has been with the Department of Bioengineering, University of Pennsylvania, Philadelphia, PA, USA, where he is currently Professor Emeritus. He has been involved in studies on the interaction of nonionizing radiation and biological systems, including mechanisms of interaction and biomedical applications of radio frequency and microwave energy. In addition, he has written widely about scientific issues related to possible health effects of electromagnetic fields. He has authored approximately 170 technical papers in peer-reviewed journals, numerous other articles, and two books related to technological risk and the law. In 2016 he received the d’Arsonval Award from the Bioelectromagnetics Society for contributions to the field of bioelectromagnetics. He is a longtime member of TC 95 of the IEEE International Committee on Electromagnetic Safety (which sets safety limits for radiofrequency energy) and a member of the Physical Agents Committee of the American Conference of Industrial Hygienists, among many other professional activities. He is Life Fellow of the IEEE, and fellow of the American Institute for Medical and Biological Engineering and the Electromagnetic Academy.
 Dr. Chung-Kwang (C-K.) Chou received his B.S. degree from National Taiwan University, in 1968, M.S. degree from Washington University, St. Louis, in 1971, and Ph.D. degree from the University of Washington, in 1975. After spending a year as an NIH Post-Doctoral Fellow with the Department of Physiology and Biophysics, University of Washington, he became a faculty member with the Department of Rehabilitation Medicine and the Center for Bioengineering, University of Washington, 1977 to 1985. From 1985 to 1998, he was a Research Scientist and the Director of the Department of Radiation Research with the City of Hope National Medical Center, Duarte, CA. In 1998, he joined Motorola, and became the Director of the Corporate EME Research Laboratory. He was the Chief EME Scientist with Motorola and Motorola Solutions from 2001 to 2013. He retired from Motorola Solutions at the end of 2013 and is currently an Independent Consultant on EMF safety issues. He is currently the Chairman of Technical Committee 95 of the IEEE International Committee on Electromagnetic Safety, responsible for exposure standards from 0 to 300 GHz (2006 to present), Distinguished Lecturer of IEEE Broadcast Technology Society (2016 to present) and on the Advisory Panel of Non-Ionizing Radiation of the NCRP (2016 to present). Dr. Chou received the highest honor d’Arsonval Medal from the Bioelectromagnetics Society in 2006 and received the IEEE Standards Association Lifetime Achievement Award in 2020. He was elected as IEEE Fellow in 1989, and also a Fellow of the American Institute for Medical and Biological Engineering in 1996 and the Electromagnetic Academy in 2007.
Dr. Chung-Kwang (C-K.) Chou received his B.S. degree from National Taiwan University, in 1968, M.S. degree from Washington University, St. Louis, in 1971, and Ph.D. degree from the University of Washington, in 1975. After spending a year as an NIH Post-Doctoral Fellow with the Department of Physiology and Biophysics, University of Washington, he became a faculty member with the Department of Rehabilitation Medicine and the Center for Bioengineering, University of Washington, 1977 to 1985. From 1985 to 1998, he was a Research Scientist and the Director of the Department of Radiation Research with the City of Hope National Medical Center, Duarte, CA. In 1998, he joined Motorola, and became the Director of the Corporate EME Research Laboratory. He was the Chief EME Scientist with Motorola and Motorola Solutions from 2001 to 2013. He retired from Motorola Solutions at the end of 2013 and is currently an Independent Consultant on EMF safety issues. He is currently the Chairman of Technical Committee 95 of the IEEE International Committee on Electromagnetic Safety, responsible for exposure standards from 0 to 300 GHz (2006 to present), Distinguished Lecturer of IEEE Broadcast Technology Society (2016 to present) and on the Advisory Panel of Non-Ionizing Radiation of the NCRP (2016 to present). Dr. Chou received the highest honor d’Arsonval Medal from the Bioelectromagnetics Society in 2006 and received the IEEE Standards Association Lifetime Achievement Award in 2020. He was elected as IEEE Fellow in 1989, and also a Fellow of the American Institute for Medical and Biological Engineering in 1996 and the Electromagnetic Academy in 2007.