{kind=link}
I’ve discussed several times over the several years that I’ve been writing for this blog my impression that the media have become in general less tolerant of antivaccine views. At least, the media seem less willing to indulge in “tell both sides” false equivalence. I remember how, back when I started blogging (a history that predates this blog by over three years), I routinely used to bemoan how news stories about vaccines or autism would almost inevitably include obligatory quotes from antivaccine activists like J.B. Handley, Jenny McCarthy, and sometimes even the Dark Lord Antivaxer Andrew Wakefield himself. I don’t know if it’s confirmation bias or reality, but over the last five years or so such tropes seem a lot less common to me. I don’t have any solid evidence to back up my impression, but I’m not alone in it. I’d like to think this decline in airing antivaccine views in the mainstream media is because evidence won out, but generally I’ve attributed much of this change to the downfall of the aforementioned Dark Lord Antivaxer Andrew Wakefield. When Wakefield lost his medical license and then was revealed to be a fraud, it provided a handy shorthand script for the mainstream media to dismiss antivaccine views without having to try very hard to explain the evidence. It’s not my preferred way to have won people over, but for most human beings stories tend to be much, much more effective than evidence for changing minds. Like it or not (and I don’t like it), discrediting a key figure of the antivaccine movement was far more effective in changing the narrative in the press than dozens of studies failing to support a link between vaccines and autism.
It’s against that backdrop that I came across a story about a study examining how the mothers of unvaccinated children are viewed by other people. Here’s the story in the Vancouver Sun:
Mothers of unvaccinated children are judged harshly by other people and their children are more likely to be shunned by other families, according to a study from the University of B.C.
And it really matters why the child is unvaccinated.
Those moms who outright refuse to vaccinate their kids are viewed most negatively, said co-author Nicholas Fitz, now a research associate at Duke University in Durham, N.C.
“On measures of social distance — like would you let your child befriend an unvaccinated child or work on a school project together — across the board unvaccinated children suffered from stigma,” he said. “People felt the most anger and the least sympathy for the refusal group and viewed the mothers as a danger to the community.”
But, because of the perceived health hazard, the child is most likely to be shunned.
“They don’t want the family to move into the neighbourhood … and they don’t want their children to play with (unvaccinated) children,” he said.
The authors Carpiano et al discuss how parents in the US are frequently judgmental of each other in the introduction to their study and then point out that vaccination status has become another area where judgmental attitudes can come into play:
In addition to these cultural expectations, media coverage of undervaccination has heavily focused on “anti-vaxxer” parents (mostly mothers), who refuse vaccinations for their children. This small, but vocal proportion of parents of the total undervaccinated population—more likely to be white and higher SES and thus with greater capacity to undertake healthy practices—are (a) known for rejecting certain evidence-based medical recommendations, (b) engaging in emotionally-, time-, and (often) financially-absorbing “intensive mothering” practices centered extensively on managing a child’s development; as well as (c) often identifying with essentialist notions of mothers as the best caregivers for their children (Reich, 2016 ; Hays, 1998). Popular media has even characterized anti-vaxxers as dangerous (e.g., Sriram, 2015). This attention paid to anti-vaxxers has contributed to misconceptions and even stereotypes about other vaccine-hesitant parents who refuse or delay vaccinations for their children (e.g., Haelle, 2015).
Of course, all antivaxers are dangerous to some extent, but there’s one message I always try to impart: It’s important to distinguish between vaccine-hesitant parents who have fallen under the sway of antivaccine views and become anxious or alarmed about vaccines and hard core antivaxers themselves, who tend to be evangelical in spreading their message. The former can be reached; the latter are virtually unreachable (with very rare exceptions).
In the study by Carpiano et al itself, the authors consider three issues:
- Is undervaccination stigmatizing for the parent and the child?
- Do stigmatizing attitudes depend on the reason for undervaccination?
- What are the policy consequences of undervaccination attitudes?
Guided by these issues, the authors sought to investigate three questions:
- To what extent does the causal reason for a child’s undervaccination status predict people’s: a. Evaluations of child undervaccination (in terms of attribution theory-based emotional reactions and/or mother judgment-based differentness, credibility, and dangerousness) and b. Stigmatizing behavioral orientations (i.e. social distance and discrimination) towards undervaccinated children and their parents?
- Do people’s evaluations of child undervaccination explain differences in stigmatizing orientations observed across different undervaccination reasons?
- Do these undervaccination evaluations and stigmatizing orientations predict support for specific child vaccination policies?
Carpiano et al examined these questions by designing a survey-embedded vignette experiment that was administered in 2015 using Amazon’s Mechanical Turk (MTurk), an online crowdsourcing Internet marketplace that allows individuals and businesses (referred to as Requesters) to coordinate the use of human intelligence. It’s a tool that’s been increasingly used to recruit subjects for social science experiments like this one. Carpiano et al designed a survey-embedded vignette experiment with checks for whether or not the participants paid attention to the instructions and had understood the survey items. Overall, the sample surveyed included 1,469 participants representing at least 46 US states and Washington, DC.
The four vignettes were about a mother who either has:
- Concerns about vaccinations and has decided to refuse vaccinations for her child (“refusal”).
- Concerns about vaccinations and has decided to delay some of her child’s vaccinations (“delay”)
- No concerns about vaccinations but whose job and family demands have made it difficult to schedule medical appointment so her child has only received some vaccinations (“time constraint”)
- No concerns about vaccinations and has decided that her child always receives recommended vaccinations (“up-to-date;” the control condition).
Because this is the age of Donald Trump, the mother in each vignette was randomized to be:
- either white (and named “Molly”) or Hispanic (and named “Maria”)
- either high or low socioeconomic status (in terms of education and job).
The authors note:
We selected Hispanic (versus White) because, in addition to Hispanic being a minority demographic group in the US, at the time we developed the study (i.e. following the Disneyland measles outbreak), politicians and pundits had publicly raised concern about illegal immigrants (often portrayed as being Hispanic) being unvaccinated and thus posing a risk for spreading disease (e.g., see Kessler, 2015). Hence, randomizing the mother’s demographics enabled us to determine if they influenced respondents’ reactions to the undervaccination condition at hand. As further context, US White and Hispanic children ages 19–35 months had similar 2014 national coverage rates for most vaccines and dosages (Hill et al., 2015).
The authors then asked questions about how the parents in the vignettes were viewed, stigmatizing behavioral orientations, and policy support. Results of evaluation measures for the vignette parents are shown in this figure:
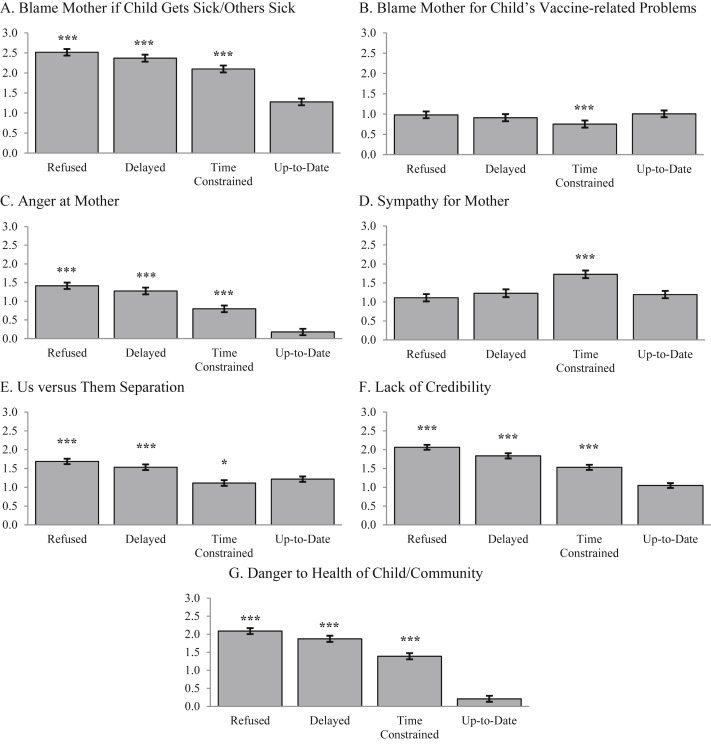
Basically, undervaccination reflected negatively on the mother. Anger and blame at the mother were highest for mothers refusing vaccines, less so for mothers who were time-constrained. These time-constrained parents also evoked much more sympathy than the other groups, which makes intuitive sense.
Here are the results on stigmatization:
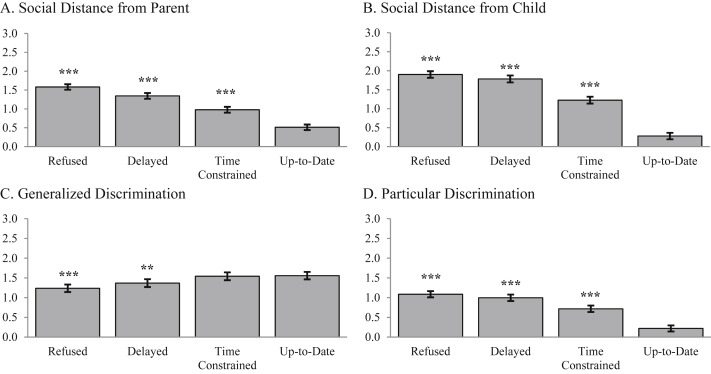
What these results suggest is that both unvaccinated children and their parents are socially stigmatized, but that the child is stigmatized more than the parents, as the differences in the scores between fully vaccinated children and the undervaccinated were much greater than the differences in stigmatization between the parents. The authors themselves note in the discussion:
Third, participants reported even stronger social distancing attitudes towards the undervaccinated child than the mother. This suggests that children bear the bigger burden in undervaccination—in addition to not being protected from one or more vaccine-preventable diseases, they may be the recipients of courtesy stigma via the stigma of their parent’s decision/inaction (Phelan et al., 1998). We further discuss this idea below in relation to advancing stigma research.
It also turns out that those who read different vignettes also ended up with different attitudes towards what should be done to encourage vaccination. Those who read the refusal vignettes tended to be more supportive of punitive measures, such as banning unvaccinated children from school, but the differences were not large. For instance, those who read the vaccine refusal vignette were only 24% more likely to support banning undervaccinated children from school. In addition, those who read the delay condition were only 15% more likely to support more education and services and 16% more likely to support reporting school vaccinated rates, while those reading the time constraint condition were 30% less likely to support a fine or a tax on parents of undervaccinated children.
So basically, the results of this study show that negative portrayals of antivaxers might actually be having an effect. However the message is being received, via the media, the Internet, or other sources, the parents of undervaccinated children are viewed negatively, and the reason matters. Outright refusers are viewed the most negatively (as they should be), and time-constrained parents the least negatively. The latter group even provokes a fair measure of sympathy. These results do not bother me. The result that does bother me is the finding that undervaccinated children are stigmatized more than the parents. This finding bothers me because it is not the children’s fault that they were born to parents who won’t protect them from infectious disease, whatever the reason for their refusal or delay of vaccines. Basically, it’s not the fault of the child of antivaxers (i.e., the “refusal” group) if his parents are pseudoscience-believing, conspiracy mongering dolts.
The authors, to their credit, tackle the issue head on. They note that social stigmatization can work in changing behavior, noting the most obvious example, smoking. They then point the similarities and differences between smoking and vaccine policies:
Our investigation also informs stigma research more generally. First, it highlights the interplay of evaluations and consequences for the parent and child. Stigma research has considered how family members of stigmatized persons can also be stigmatized as recipients of courtesy stigma (Phelan et al., 1998). Child undervaccination extends the courtesy stigma concept, as the focus of the stigma is both the parent and the child—for mutual and distinct reasons. A child’s (under)vaccination status is a consequence of the parent’s actions, regardless of whether those actions are by choice or constraint. This status is beyond a child’s control, yet the child bears the burden of any negative consequences from parental (in)action. Thus, the child risks being doubly stigmatized as both the identified child of a vaccine-hesitant parent and a perceived health risk.
Second, our focus on stigma of undervaccinated children and their parents provides important angles to scholarship on the ethics of using stigma (or more broadly, denormalization) as a policy tool for modifying behaviors (see debates between Bayer, 2008a ; Bayer, 2008b and Burris, 2008; and Bell et al., 2010 ; Bayer, 2010). Given that vaccinations are necessary for ensuring the health of a community (including people who cannot be vaccinated), they juxtapose individual and public rights (as well as the role of government). This situation is similar to anti-smoking policies and second-hand smoke, but is more complex in that it entails the parent (as the decision maker) and child (as a beneficiary and health risk). This additional dimension is essential in ongoing debates about stigma and policies that aim to address adult and child health conditions and behaviors (e.g., eating unhealthy foods, obesity).
Of course, hard core antivaccine parents feed on any perception of stigmatization. How often have you read posts by such parents ranting about how they feel judged when interacting with health care providers, the press, and others? They revel in painting themselves as the persecuted minority, sometimes going to ridiculous extremes, such as donning a yellow badge with a syringe on it patterned after the Yellow Star of David that the Nazis required Jews to wear, thus likening their “plight” to that of the Jews during the Holocaust. Indeed, antivaxers are quite enamored of Holocaust analogies, either with vaccines causing a Holocaust or laws requiring children to be vaccinated before they can attend school being likened to Nazi-ism. Even mildly vaccine-hesitant parents can be turned off by excessive judgment.
Basically, stigmatization is highly problematic because it is the children who suffer from it far more than the parents, even as they are left unnecessarily vulnerable to infectious diseases. Also, we basically know that stigmatization only makes the beliefs of committed antivaxers stronger and increases their will to resist. However, this group of antivaxers is, as I pointed out at the beginning, different from the mere vaccine-averse, who are far more numerous. The numbers of hard core antivaxers are smaller, even though they are much louder and more responsible for spreading antivaccine beliefs.
The real question is whether stigmatization has an effect on vaccine-hesitant parents and whether it makes them more or less likely to vaccinate—and at what cost, given that it is the children who suffer far more than the parents. While it’s encouraging that parents of undervaccinated children are not viewed favorably because it suggests that in our society pro-vaccination views predominate and that the reason for not vaccinating matters, we have to ask: How can we as a society maximize the social pressure to vaccinate without harming the very children that suffer from not being vaccinated? The answers to those questions await further research.