{kind=link}
Unkind, largely unqualified, and highly judgmental
My Twitter bio reads that I am “unkind, largely unqualified, and highly judgmental.” This colorful description comes courtesy of Professor Francis Balloux, the chair of computational biology at the University College London. I earned this opprobrium for saying that while there are many viruses (HPV, VZV, HBV, HIV, polio) with sequelae that emerge after the initial infection, I was generally not aware of such long-term side effects from vaccines. Professor Balloux disagreed, saying my comment was,
So extraordinarily uninformed in the context of COVID-19 that it belongs in the league of “SARS-CoV-2 has never been isolated”, “the vaccine alters your DNA”, “Omicron is a mutant hybrid between a coronavirus and rhinovirus” takes.
My position is that SARS-CoV-2 is a new virus and we have to be humble about the possibility of long-term consequences, especially compared to the vaccine. I want to error on the side of caution. If someone feels I am unkind, largely unqualified, and highly judgmental for this reason, I am prepared to live with their condemnation.
Beyond this, Professor Balloux said that I was “threatening” him when I announced my intention to write this essay. I wrote previously how histrionically labeling potential written criticism as “threatening” is itself an attempt to pre-emptively silence or discredit one’s critics. It can be very effective. Who wants to be seen as “threatening” a famous professor who has advised top government officials? Not me. I don’t ever want to be seeing as threatening anyone.
But everyone can relax. None of my previous essays contained any threats, and this one is no different. Rather, I’m just going to share my thoughts on a few of Professor Balloux’s tweets. That’s it.
“Healthy kids have to be exposed to the virus, ideally earlier than later”
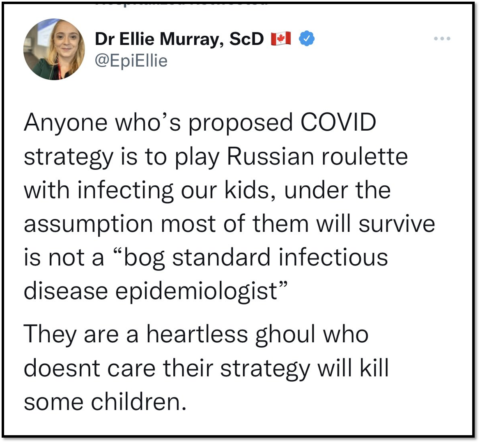
With this in mind, let’s examine the first of those tweets. It said:
I’m not sure how to convey this message in a half-acceptable way. But, if the objective were to send SARCoV2 into endemicity, then healthy kids have to be exposed to the virus, ideally earlier than later. This is not ‘eugenism’; it is bog-standard infection disease epidemiology.
“A disease can be endemic and both widespread and deadly”
First let’s talk about the use of the word “endemicity” here, because it sure seems as if Professor Balloux believes this is a very desirable goal. To my reading at least, he gives the impression that things might be much better if we can only “send SARCoV2 into endemicity”. Of course I hope this is true, but not every epidemiologist sees it this way. In a sobering essay called “COVID-19: Endemic Doesn’t Mean Harmless“, Dr. Aris Katzourakis, a professor who studies viral evolution and genomics at the University of Oxford, wrote:
The word ‘endemic’ has become one of the most misused of the pandemic. And many of the errant assumptions made encourage a misplaced complacency. It doesn’t mean that COVID-19 will come to a natural end.
To an epidemiologist, an endemic infection is one in which overall rates are static — not rising, not falling. More precisely, it means that the proportion of people who can get sick balances out the ‘basic reproduction number’ of the virus, the number of individuals that an infected individual would infect, assuming a population in which everyone could get sick. Yes, common colds are endemic. So are Lassa fever, malaria and polio. So was smallpox, until vaccines stamped it out.
In other words, a disease can be endemic and both widespread and deadly. Malaria killed more than 600,000 people in 2020. Ten million fell ill with tuberculosis that same year and 1.5 million died. Endemic certainly does not mean that evolution has somehow tamed a pathogen so that life simply returns to ‘normal’.
Basically, endemic COVID-19 might still be dangerous COVID-19, the way endemic measles infected, hospitalized, and even killed children every year before the vaccine.
“This makes no sense, and is hard to distinguish from anti-vaxxer rhetoric”
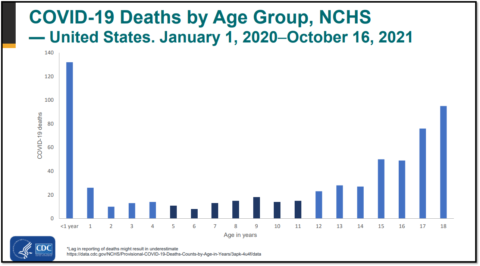
Next let’s examine Professor Balloux’s suggestion that to achieve endemicity “healthy kids have to be exposed to the virus, ideally earlier than later”. This is false. Infants have the highest risk of dying of all children. In the USA, 200 infants died from COVID-19 compared to 87 deaths in children ages 1-4 years. Doctors who actually treat children know this. Dr. Pieter Peach said:
There are some exposures to viruses that are best delayed until someone isn’t an infant with small diameter, irritable airways, or until they or their siblings have had a chance to get vaccinated against them.
Telling parents that it’s always better to expose their children to the virus “ideally earlier than later” is dangerously wrong for this reason alone. We do not want parents to falsely think that babies are entirely spared by this virus, when in fact they are the most vulnerable. Scientists who communicate with the public under the guise of being an expert on a deadly virus should strive to be accurate and thorough, even if that means being less edgy on social media.
However, Professor Balloux’s broader point is obviously true – children generally fare much better with COVID-19 than adults. Although it’s frontloading the risk, it may be preferable for people to catch some viruses as children. While I don’t think parents ever had “polio parties”, my mom exposed me to chickenpox as a child, and I don’t think she’s a sociopath. This all may make some sense in a world without vaccines.
However, this is not the blessed world in which we live! My children were vaccinated against chickenpox. They were vaccinated against COVID-19. Professor Balloux’s comment might have been perfectly reasonable had he prefaced it by saying, “were I trying to protect children from COVID-19 in the year 1767, here’s what I’d do”.
Even though it’s 2022 and we have effective vaccines, Professor Balloux did not mention them, at least not initially. I was not the only one who noticed this curious omission in his statement that “healthy kids have to be exposed to the virus, ideally earlier than later”. Many people pointed out that actually, healthy children don’t have to be exposed to the virus right now. They can be vaccinated first.
Dr. Stephen Griffin voiced this sentiment by saying:
No Francois, that is an appalling statement. You may have said this to provoke debate, but how can you seriously advocate putting children in harms way when there’s a safe and effective vaccine available? These are not numbers, these are children, including vulnerable kids.
He’s right.
Someone else commented:
The reason you can’t think of an acceptable way to convey this, is that it is not acceptable. It is also not standard epidemiology. We have safe and effective vaccines. This makes no sense, and is hard to distinguish from anti-vaxxer rhetoric.
He’s right too. I’ve read a ton of anti-vaxxer rhetoric. The notion that “healthy kids have to be exposed to the virus, ideally earlier than later” would not seem at all out of place in an anti-vaccine essay. If you wanted to tweak Professor Balloux’s tweet to convince a friend it came from an anti-vaccine super crank like Dr. Joseph Mercola, what exactly would you change? Very little it seems. In fact, Dr. Mercola wrote that, “having healthy, unvaccinated children in the population is crucial to achieving herd immunity”. Of course, getting immunity to the virus by getting the virus is a bit like giving away all your money to ensure nobody ever robs you. It works, but…
“You may have failed to understand because you’re not an infectious disease epidemiologist. I didn’t comment on child vaccination.”
In response to his many critics, Professor Balloux said that his “point was not whether healthy children should be vaccinated against Covid or not”. He further explained to a critic that:
You may have failed to understand because you’re not an infectious disease epidemiologist. I didn’t comment on child vaccination. I just stated that SARSCoV2 becoming endemic would imply children being exposed, and earlier would be better than later given the age risk profile.
Well, I’m not an infectious disease epidemiologist either, so maybe I am failing to understand too, but this strikes me as an odd statement. Is there a secret oath of silence that forbids infectious disease epidemiologists from commenting on child vaccination? I doubt it, especially considering there is robust evidence that the vaccine can prevent rare, but catastrophic outcomes in adolescents. To me, discussing vaccines sounds like part of the core job description of infectious disease epidemiologists, especially when they communicate with the general public on social media.
Professor Balloux announced his intention to respond to my essay. I won’t say he is “threatening” me when he writes his rebuttal, “No, An Infectious Disease Epidemiologist Shouldn’t Comment on Child Vaccination“. I look forward to learning the reasons why an infectious disease epidemiologist should not comment on child vaccination when discussing a virus for which an effective vaccine exists. Maybe I’ll learn something.
“Vaccinating healthy ≤12 year olds makes hardly difference to them directly”
Assuming there is no infectious disease epidemiologist code of omertà regarding child vaccination, this raises an important question. Why would someone refuse to comment on child vaccination when an extremely effective vaccine exists? If a patient was diagnosed with a condition that carried a low, but non-zero risk of serious illness or even death, his doctor would be guilty of obvious malpractice if she neglected to tell him there was a safe and effective treatment. The negligence would be compounded if, when asked about that specific treatment, the doctor said it was unnecessary.
This brings me to the final tweet I will discuss. In response to a questioner who asked “with all due respect, why are we exposing them before vaccinating them?” Professor Balloux responded:
This is an interesting question. Vaccinating healthy ≤12 year olds makes hardly difference to them directly, however we look at it. It has some indirect impact on the dynamic of the pandemic, though. It all depends on what we hope to maximise/minimise.
This is an interesting question, but not for the reasons Professor Balloux thinks. The questioner was right. We are exposing many children to the virus before we are vaccinating them. Why are we doing this?
We are doing this because some influential people don’t care if children get the virus, while other influential people actively want children to get the virus. Professor Balloux was absolutely right when he said “It all depends on what we hope to maximise/minimise”. I very much want to minimize the number of children who encounter this virus before they are vaccinated. Other people very much want to maximize this number.
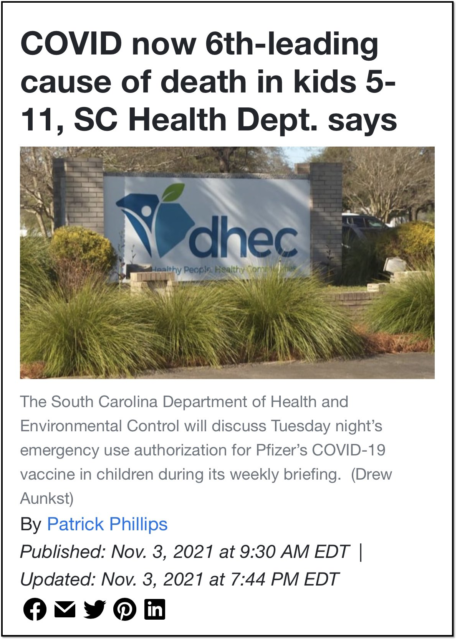
There is a bizarre and dangerous line of thought that it is beneficial for children to get COVID-19. As far as I know, this notion originated early in the pandemic when Dr. John Ioannidis lamented that children might avoid the virus saying, “school closures may also diminish the chances of developing herd immunity in an age group that is spared serious disease”.
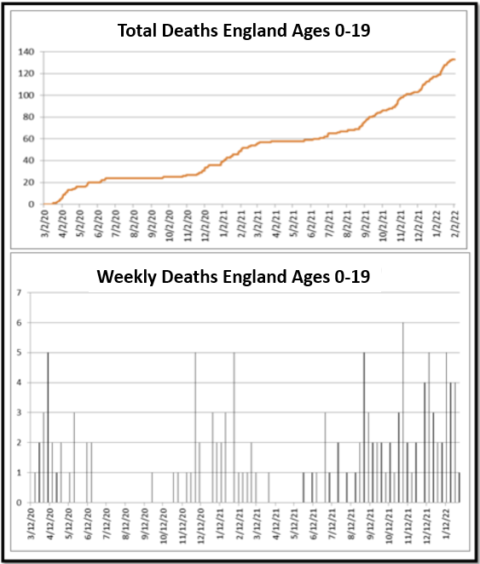
According to the CDC’s COVID Data Tracker, 1,247 American children have died since Dr. Ioannidis made that statement, and over 100,000 children have been hospitalized, some of them very sick, needing mechanical ventilation in the ICU. There have been 6,851 cases of MIS-C. Up to 80% of these children require treatment in the ICU. MIS-C has killed 59 children. A great many people refuse to acknowledge these grim numbers, which would have been much higher had nothing been done to “diminish the chances of developing herd immunity” in children.
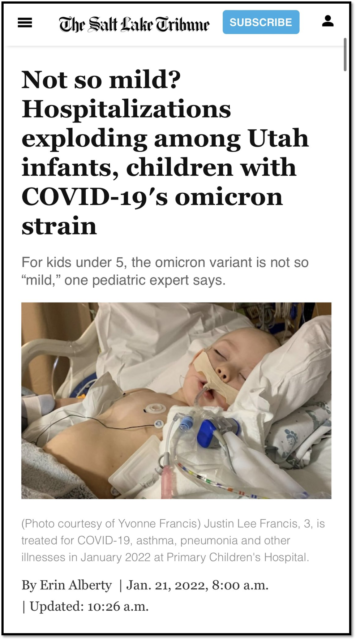
The movement to infect children was formalized in the pro-virus Great Barrington Declaration, which now opposes vaccinating children. Unfortunately, this group has been very successful. They can take a lot of credit for both low vaccination rates and high infection rates in children. Even today, after Omicron hospitalized a record number of sick children, the notion that the virus is beneficial for children still persists.
In an article called “Should We Let Children Catch Omicron?”, Drs. Vinay Prasad and Allison Krug wrote “For children, getting sick and recovering is part of a natural and healthy life”. They said that “even unvaccinated children generally do well after Covid-19 infection” and “Immunity is built through illness”. This article favorably quoted Professor Balloux’s tweet that advocated exposing healthy kids to the virus, ideally earlier than later. It did not urge parents to vaccinate their children, nor did it mention that 1,247 deceased children didn’t build immunity through illness. These type of articles never do, though the authors would bristle with disbelief if you suggested this position was in any way “anti-vaccine”.
Thankfully the idea that COVID-19 was beneficial for children carried no weight with American regulators when they issued their Emergency Use Authorization for pediatric vaccines. Unfortunately, things were different in the England. As I discussed previously, some members of the Joint Committee on Vaccination and Immunisation advocated using infected children as a means to “boost immunity in adults through exposure”. They said “natural infection in children could have substantial long-term benefits on COVID-19 in the England”. I meant it when I said there are people who believe it is beneficial for children to get COVID-19. In August 2021, Professor Balloux endorsed the JCVI’s decision not to vaccinate children, saying “I think the JCVI has probably been right to err on the side of caution”.
To be clear, the JCVI erred on the side of the virus, not on the side of caution. There is nothing cautious about letting a novel virus run rampant in children when an effective vaccine is available to them. Predictably, in October 2021, the headlines declared “Children Drive Britain’s Longest-Running Covid Surge“. Unvaccinated children are currently getting sick and missing school in England. Just like in the US, the virus, not fantasized lockdowns, disrupted schools, though cases are thankfully dropping fast here. Children in England suffered more this winter than any time during the entire pandemic.
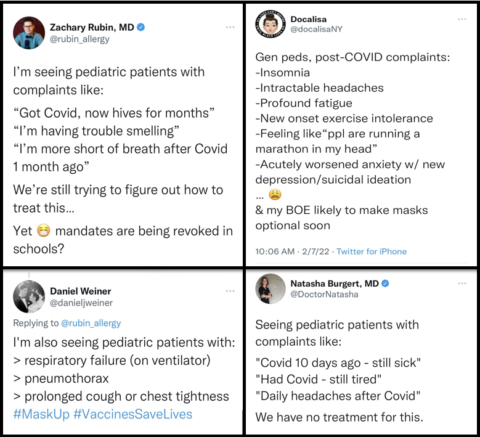
Meanwhile, there is very preliminary evidence that, like many viruses, SARS-CoV-2 might lead to long term complications in some children after all, namely diabetes. We have a lot to learn about this virus. Doctors who actually treat sick children see it this way too. Their dedication to children strikes me as kind, extremely qualified, and not at all judgmental. To rule out the potential of prolonged COVID-19 symptoms in children is basically to call these doctors and their patients liars. Not all children feel 100% back to normal after having COVID-19, though most do.
Vaccinating children is erring on the side of caution
Anyone who wants to err on the side of caution would strongly advocate vaccinating children. The vaccine was safe and effective in preventing SARS-CoV-2 infection in children ages 5-11 years in the clinical trial, though it was not large enough to show that the vaccine prevented severe outcomes or to detect rare side effects. Not enough time has elapsed to collect and synthesize much real-world data regarding the efficacy of the vaccine in children this age. It took several months before that data emerged in adolescents, but there now are multiple studies showing the vaccine is effective in keeping them healthy and out of the hospital.
Those who communicate about children and COVID-19 should be extremely eager to share this vital information with the public. It’s really very easy to do.
- Study 1: In hospitalized adolescents, “179 COVID-19 case-patients, six (3%) were vaccinated and 173 (97%) were unvaccinated. Overall, 77 (43%) case-patients were admitted to an intensive care unit, and 29 (16%) critically ill case-patients received life support during hospitalization, including invasive mechanical ventilation, vasoactive infusions, or extracorporeal membrane oxygenation; two of these 29 critically ill patients (7%) died. All 77 case-patients admitted to the intensive care unit, all 29 critically ill case-patients, and both deaths occurred among unvaccinated case-patients.”
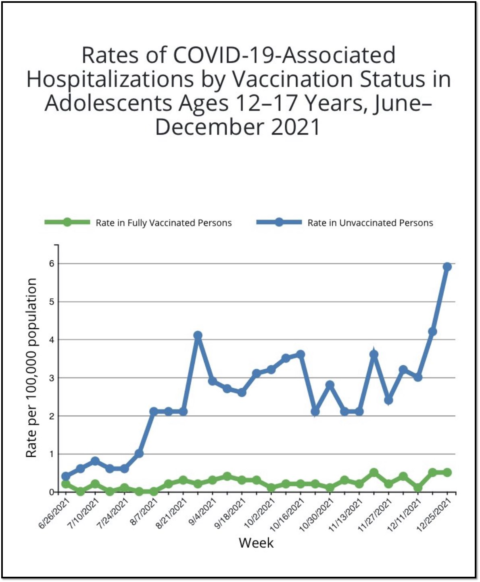
- Study 2: “Hospitalization rates were 10 times higher among unvaccinated than among fully vaccinated adolescents.”
- Study 3: “Among 272 vaccine-eligible (aged 12–17 years) patients hospitalized for COVID-19, one was fully vaccinated.”
- Study 4: Vaccine effectiveness “was 92% against SARS-CoV-2 infections irrespective of symptom status.”
- Study 5: “97/102 children with MIS-C were unvaccinated. None of the 5 vaccinated MIS-C patients required respiratory or cardiovascular life support (invasive mechanical ventilation, vasoactive infusions, or ECMO) compared to 38/97 unvaccinated MIS-C patients.”
- Study 6: “In 33 adolescents with MIS-C eligible for vaccination, “0 had been fully vaccinated, 7 had received 1 dose.”
- Study 7: “Of the case patients, 180 (40%) were admitted to the ICU, and 127 (29%) required life support; only 2 patients in the ICU had been fully vaccinated. The overall effectiveness of the BNT162b2 vaccine against hospitalization for Covid-19 was 94%. The effectiveness was 98% against ICU admission and 98% against Covid-19 resulting in the receipt of life support. All 7 deaths occurred in patients who were unvaccinated.”
“Caution” isn’t always cautious
In case you just skimmed those studies, I’ll highlight that essentially all children who needed life support were unvaccinated, and all children who died were unvaccinated. It’s a scandal that so many contrarian doctors have pontificated profusely about the dangers of vaccinating children without even mentioning these studies exist. A lot of parents don’t know how effective these vaccines are at keeping children safe. Their pandemic sources only discuss one thing, and it’s not any of the seven studies above.
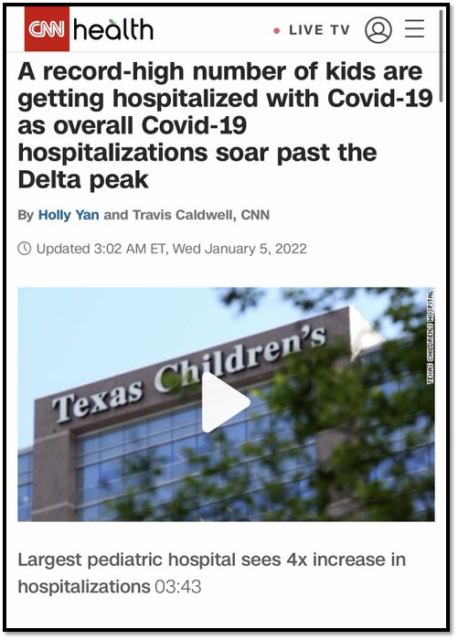
Data about the vaccine for younger children is emerging, and unsurprisingly it parallels data for adolescents. Pediatricians across the country are saying the same exact same thing – it is unvaccinated children who are being hospitalized with COVID-19. For example, a children’s hospital in Texas reported that “of all the pediatric COVID patients they admitted in January, 91% had not been vaccinated”. Of course, not enough children have been vaccinated, and that’s the problem.
During New York’s recent Omicron surge 91% of 5- to 11-year-olds who were hospitalized with COVID were unvaccinated (20% of the children that age were fully vaccinated overall). 54% of children admitted to the hospital had no comorbidities, and there were very few incidental admissions. Vaccinating these healthy children absolutely would have made a difference to them directly, and anyone who claims otherwise is wrong.
Moreover, the vaccine is incredibly safe in children under 12. After 8.7 million vaccine doses, there were just 11 verified myocarditis cases. 7 of these children have recovered and 4 were “recovering”. No child in the entire world has died from the vaccine as far as I know.
The vaccine has absolutely saved the lives of some healthy American children and prevented many more from being hospitalized. I suspect that when we look back at the decisions regulators made this pandemic, the generally slow pace in authorizing vaccines for children older will be seen as a mistake.
I recognize regulators have an impossible job. They’ll be second guessed by social media stars with no real-world responsibility no matter what they do. While regulators need to wait to ensure that vaccines are safe and effective, there is also a price for prolonged waiting. Children under 5 years can still not get vaccinated, though I am hopeful that we will soon see data showing the vaccine prevents COVID-19 in children this age.
Sadly, COVID-19 spread rapidly through children this winter, and the Omicron variant took a nasty toll on many young children this winter. Remember, 200 infants have died of COVID-19. The American Academy of Pediatrics added 21 children to its grim death tally this week alone, as it has basically every week for the past 6 months.
“Caution” isn’t always cautious.
The vaccine will make all the difference to some children
The claim that vaccinating “healthy ≤12 year olds makes hardly (any) difference to them directly” would be true if COVID-19 posed zero risk to healthy children or the vaccine were useless. Again, this is not the world in which we live. The vast majority of children do just fine with COVID-19, especially healthy children, but not all. Given that millions of children have been infected in the UK and USA, these rare harms have added up. It’s true that the vaccine won’t make a difference to most children.
But it will make all the difference to some children.
Many arguments against vaccinating children simply boil down to, the vaccine won’t save the lives of that many children, so there’s really no point. I don’t think that’s a very good argument, especially considering about 20% of COVID-19 deaths are in healthy children, and healthy, unvaccinated children have died of COVID-19 after the vaccine was available.
Standard anti-vaccine blather
Arguing that vaccines are unnecessary since the diseases they prevent harm only a very small percentage of children is standard anti-vaccine blather. In fact, I’d argue that the two central pillars of anti-vaccine ideology are that vaccines are dangerous while the diseases they prevent are benign. For example, Dr. Mercola stated in his anti-vaccine article that COVID-19 is a disease with “practically zero risk of dying from as a child or adolescent”.
Does this sound familiar? It will if you’ve read anything I’ve written here before. Every doctor I’ve criticized here previously has said essentially the same thing. Like Dr. Mercola, these doctors long ago chained themselves to the idea that “COVID is mild for children,” and even after 1,247 deaths and 100,000 hospitalizations, there’s nothing that can shake that belief.
It may be true that any individual child’s risk of dying of COVID-19 is “practically zero”, but there’s a world of difference between “practically zero” and actually zero when tens of millions of children get infected. 1,247 dead children is a tragically large number of dead children, which is why the doctors I’ve criticized never share that number. Neither does Dr. Mercola. Unbelievably, they all still insist on comparing it to the flu, a disease that killed 6 children during this year. We vaccinate children against the flu. Most of us don’t want any child to die because the missed a vaccine. This is not a very controversial opinion.
Moreover, the argument that vaccinating healthy children “makes hardly difference to them directly” could be said of many vaccine-preventable diseases. If all vaccines vanished tomorrow, most kids, especially healthy ones, wouldn’t die. The vast majority of kids who contracted measles, rubella, mumps, HPV, VZV, and even poliovirus did not suffer grave harms. Yet, once vaccines for these viruses because available, it became bog-standard infectious disease practice to give them to children, thankfully. These vaccines have spared much suffering for children and their families. So has the COVID-19 vaccine.
At this point, what difference is there really between someone who denies the value of other vaccines and someone who denies the value of just the COVID-19 vaccine? Not much that I can see. Other vaccines have a much longer safety profile and that matters, but COVID-19 is circulating right now. Millions of American children have gotten COVID-19 this year, compared to zero measles cases so far. If the parent of an unvaccinated child was only willing to get one vaccine for his child, the MMR or the COVID-19 vaccine, I’d suggest the COVID-19 vaccine in a heartbeat.
Fortunately, pediatric hospitalizations are declining from their peak, when just under 1,000 children were hospitalized daily. Still, a large number of children have yet to contract the virus, and it is never going away. We should do everything we can to protect children with the vaccine, not undermine this effort. It’s a tragedy that pediatric vaccination rates are so low.
“We should have zero tolerance for any school-aged child to develop severe COVID”
Of course infectious disease epidemiologists are allowed to talk about child vaccination. Most of them do. They’re the ones who don’t need to clarify that their ideas aren’t “eugenism”.
In contrast other people decide not to share information about the vaccine. It’s a choice they make. Sadly, when it comes to children, many people, who claim to value “nuance” and “centrism” refuse to share any bad news about the virus or any good news about the vaccine. As I discussed previously, there absolutely is a code of silence about the potential dangers of the virus and the successes of the vaccine for children. However, those who abide by this code are not infectious disease epidemiologists, but rather contrarian doctors and scientists who will never work in a pediatric ICU, taking care of an intubated child. Sick children seem to be an abstraction for them, numbers on government websites.
I disagree. As Dr. Carter Mecher told me:
Pediatric deaths deserve special mention. Talk to any parent who lost a child for any reason. I’m not sure that they ever fully recover from that grief. We have a word for who is left behind when a spouse dies. We have a word for who is left behind when a parent with children dies. But we have no word for a parent left behind when a child dies.
He’s right. Imagine how upsetting it would be to have lost a child to COVID-19 and to constantly encounter highly-visible doctors and scientists – who don’t treat sick children – relentlessly minimize the virus that killed her at every opportunity. Wouldn’t it just be easier to encourage parents to vaccinate their children than to come with bizarre rationalizations as to why 1200 = 6?
Sadly, it’s easy for some people to minimize young victims of COVID-19 as long as they remain an abstraction. This all changes when someone uses their exact language to minimize a virus that affected someone in their family. It’s a horrible thing to lose a loved one to a terrible disease like AIDS.
It’s also a horrible thing to lose a loved one to a terrible disease like COVID-19. Dr. Griffin was right when he said, “These are not numbers, these are children, including vulnerable kids”. These children were someone else’s sisters and brothers. According to news reports, the sister of Jorja Halliday, a teenager who died from COVID-19 “says she cries herself to sleep every night, as she described the shock of losing her older sibling”. She looks too young to curse.

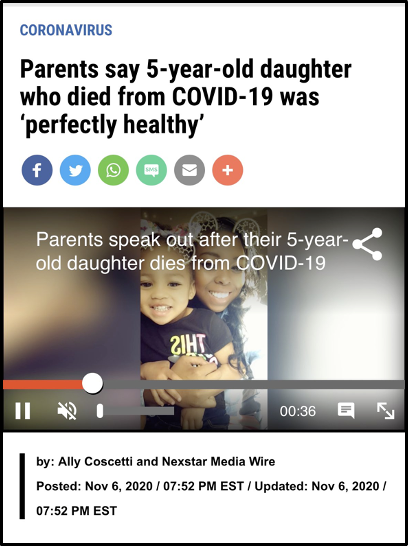
It’s worth it to read about some of the deceased children and the regret their parents feel about not vaccinating them. Landon Woodson’s mother implored parents to “Please Please Get Vaccinated“, after her son, a healthy football player, died of COVID-19. Similarly, Hector Ramirez, whose unvaccinated 15-year-old-daughter Victoria died this summer, said:
I don’t want any other parent to go through what I did — seeing my daughter perfectly healthy one day, then following a week and a half, she’s gone.
According to news reports, “He didn’t get the shot for his daughter, and he regrets it”.
Teresa Sperry’s parents became vaccine advocates after their daughter, who was not yet eligible to be vaccinated, died of COVID-19. “The only way this makes sense to me is if it saves people”, Jeff Sperry said. “We’re trying to help others so they don’t have to go through this”. Imagine how they must feel to see prominent scientists on social media, divorced from patient care, constantly undermine their effort.
The vaccine would have made a big difference to Landon, Victoria, Teresa, and many of the 81 American children or the 16 English children who died of COVID-19 in the past month. Pediatricians who actually have real-world responsibility for sick children know this. Drs. Jennifer Lighter and Stephanie Ungar recently said,
While it is reassuring that severe illness is rare in children infected with SARS-CoV-2, it can still occur. We should have zero tolerance for any school-aged child to develop severe Covid, as vaccinations have made this scenario avoidable.
It is appalling this is a controversial statement considering the overwhelming evidence it is true.
Sometimes what people don’t tell you is much more revealing than what they do
COVID-19 is here to stay. Contrarian doctors who harbored fantasies that COVID-19 would melt away, obviating the need for pediatric vaccines now instead extol the virtues of “natural immunity.” I fully agree that very few children will escape exposure to this virus over the course of their lifetimes. However, in fortunate parts of the world, their parents have a choice. Their child can encounter the virus with a vaccine or without a vaccine. The vast majority of children will be fine either way thankfully, but not all. A child’s chance of avoiding a rare but devastating harm is much lower with the vaccine.
Doctors and scientists who communicate with the public about COVID-19 and children also have a choice. They can share this fact or they can refuse to do so.
Sometimes what people don’t tell you is much more revealing than what they do.