
{kind=link}
Specific narratives of antivaccine misinformation about any given vaccine generally consist of a combination of a subset (or all) of the following elements. First, of course, the narrative must, as all antivaccine narratives do, include a conspiracy theory, such as efforts by “them” (e.g., the government, big pharma) are trying to keep “The Truth” about vaccines from the public. Second, that “truth” about the vaccine, according to antivaccine narratives, is that it is dangerous—and preferably ineffective as well. Examples are numerous, and regular readers of this blog are familiar with the harms that antivaxxers falsely attribute to vaccines; e.g., autism, autoimmune diseases, cancer, and even death. To support the narrative of harm from vaccines, antivaxxers routinely portray vaccines as laden with toxins and made with “aborted fetal tissue” and “fetal cells“. It’s not enough, though, for antivaxxers to portray vaccines as dangerous to just the people receiving them. They have to portray vaccines as dangerous to others who have not received them as well. Before COVID-19, antivaxxers tried to claim that the recently vaccinated were dangerous because they “shed” virus from the vaccine (this does happen but is not dangerous and cases of disease from vaccine shedding are exceedingly rare). Unsurprisingly, in a case of everything old being new again, antivaxxers have co-opted many of tried-and-not-true narratives and deployed them in the service of spreading fear about COVID-19 vaccines, including the claim that they are made with “fetal cells“, portraying the lipid nanoparticles in them as horrifically toxic, and the mRNA in the Pfizer and Moderna vaccines as “experimental gene therapy” that “hacks the software of life“. They’ve even falsely claimed that COVID-19 vaccines cause cancer, Alzheimer’s disease, and death. But what about shedding?
When COVID-19 vaccines based on mRNA technology were first introduced, I naively thought that antivaxxers would not be able to adapt the narrative of the vaccinated being a danger to the unvaccinated due to “shedding”, because the mRNA technology used by Moderna and Pfizer/BioNTech induces cells in the recipient only to make a single protein from SARS-CoV-2, the coronavirus that causes COVID-19. Similarly, COVID-19 vaccines based on adenovirus vectors, such as the AstraZeneca and Johnson & Johnson manufacture, simply use a different method to achieve the same goal: To produce the SARS-CoV-2 spike protein and thereby produce an immune response. None of the current COVID-19 vaccines produces a full intact coronavirus, not even a weakened one, as live-attenuated virus vaccines, such as the measles vaccine, use a weakened version of the measles virus. To summarize, current COVID-19 vaccines neither contain coronavirus, killed or live-attenuated, nor can they produce a full virus. None of this science stopped antivaxxers from adopting their narrative of “shedding” from vaccines as being a danger to those around the vaccinated. They happily started portraying the spike protein as deadly and falsely claimed that the vaccinated were “shedding” spike protein, leading to illness, menstrual disturbances, and even miscarriages in those exposed.
Over the last month, there have been three new papers that have been making the rounds among antivaxxers as “scientific proof” that not only is the coronavirus spike protein highly toxic to the vaccinated but that it is produced by the vaccinated in amounts that can cause those toxic effects. I thought I’d take some time to take a look at them. The first two papers are often presented as “slam dunk” evidence that the coronavirus spike protein is toxic and deadly (and, therefore, the COVID-19 vaccines are deadly), while the last paper is presented as evidence that mRNA vaccines produce enough spike protein to poison recipients. Spoiler alert: None of these papers show what antivaxxers represent them as showing, especially the third one.
Spike proteins and pulmonary hypertension
The first of these papers was one that I first noticed nearly a month ago on Twitter, although the study was older than that, dating back to January:
I read this; about the spike protein; that the mRNA vaccines are supposed to make in the body; and that it could cause pulmonary hypertension. I hope it’s not that. https://t.co/NdZ6CLWm5A
— Simone (@simonevdm) March 11, 2021
And here’s the study, from Georgetown and the Ukraine, “SARS-CoV-2 Spike Protein Elicits Cell Signaling in Human Host Cells: Implications for Possible Consequences of COVID-19 Vaccines“.
It turns out that this “study” isn’t even a study at all. Rather, it’s more like a “news and views” or opinion piece, a review article if you’re feeling particularly generous. Moreover, it was published in Vaccines (Basel), an open access journal in the MDPI group of journals. Unsurprisingly, MDPI journals are pretty dubious, with MDPI having been listed on Beale’s list of predatory journals in 2013. It ultimately successfully appealed and was removed from the list. However, from my perspective, I do not consider MDPI journals as being high quality and would never publish in one.
But what about the paper itself? Let’s just say that I was quite…underwhelmed…by it. Indeed, rarely in my many years of reading scientific papers have I seen so few experiments cited in a review article do such heavy lifting to provide such weak evidence for a conclusion like the claim that the spike protein can cause pulmonary hypertension.
At its essence, pulmonary hypertension is high blood pressure in the lungs. The circulatory system is divided into two components, the pulmonary system, in which blood flows through the blood vessels in the lungs, picks up oxygen, and then flows to the systemic circulation (the rest of the body) to deliver that oxygen to the tissues. The pulmonary vascular system is a much lower pressure system than the systemic circulation, which is why the right ventricle, the chamber of the heart that pumps blood through the lungs, is less muscular than the left ventricle, which pumps blood through the rest of the body. In any event, pulmonary hypertension can be caused by a number of things, including some types of congenital heart disease, connective tissue disease, coronary artery disease, high blood pressure, liver disease (cirrhosis), blood clots to the lungs, and chronic lung diseases like emphysema. The sequelae of pulmonary hypertension can be severe, including right-sided heart failure, hemorrhage in the lung, clotting, pulmonary artery dissection, and more. Let’s just say that pulmonary hypertension can be very bad.
On what do these authors base their claim that spike protein can cause pulmonary hypertension? They cite the most tenuous of evidence, and not very much of it. For instance, The first study is nothing more than a cell culture study coupled with a postmortem study of lungs first published last August, in which the authors (who happened to be them—yes, they cited their own paper) combined observations to make the leap to speculation that spike protein alone can cause the problems seen in COVID-19. In the cell culture component, the authors treated the cells that line pulmonary arteries (pulmonary artery endothelial cells) and the smooth muscle that surrounds the endothelial cells with spike protein and found that spike protein can cause intracellular signaling in these cells of a sort associated with cell injury. They also examined postmortem lung tissues from patients who died of COVID-19 and found pulmonary vascular wall thickening, a hallmark of pulmonary arterial hypertension. That’s it. No, really, that’s it. To be fair, the authors did compare the lungs of patients who died of H1N1 influenza to those who died of COVID-19 and found that the pulmonary arteries were markedly thicker in the patients who died of COVID-19. It’s an interesting observation, but if there’s one thing that was observed early in the pandemic it’s that the ARDS (acute respiratory distress syndrome) caused by COVID-19 was like nothing critical care doctors had ever seen before.
There is no more, at least not from these authors. Sure, they do cite two other papers, one from 2005 showing that injecting mice with recombinant spike protein from SARS reduced the ACE2 expression and worsened acid-induced lung injury. The other paper is from December and reports that the full-length SARS-CoV-2 spike protein activated NF-κB (a signaling pathway I’m well familiar with) and AP-1 transcription factors as well as p38 and ERK mitogen-activated protein kinases. Again, you don’t need to know the details other than that these are survival and growth pathways, but also that this observation was not made in cells from the pulmonary vasculature, but rather from a cell line (A549) from the lungs and another (Huh7.5) from the liver. The relevance of this study to whether spike protein can cause pulmonary hypertension is questionable at best.
Now that’s it: One study by the authors, two observations, one involving spike protein and one involving actual viral infection, plus an old study of SARS spike protein. I say this because it needs to be emphasized that what the authors reported was in patients who died of infection with the whole virus, SARS-CoV-2. You have to separate the effects of full infection and the effect of spike protein alone, and the authors did not do this, other than as a prelude to speculation that spike protein alone might cause pulmonary hypertension. Even for “proof” commonly cited by antivaxxers, this was weak sauce.
The deadly spike protein, take two
About three weeks ago, antivaxxers started pointing to a study from the Salk Institute as yet more “proof” that the spike protein used in COVID-19 vaccines is toxic and deadly. For instance, behold Alex Berenson, the “pandemic’s wrongest man“, crowing about the study:
As smoking guns go, this study is high-caliber. @UCSanDiego and Chinese researchers showed that the #SARSCoV2 spike protein – the one the vaccines make you produce – can all by itself cause major damage to the walls of blood vessels. pic.twitter.com/Fk5DNZugzH
— Alex Berenson (@AlexBerenson) May 2, 2021
Sorry, here: https://t.co/I3r91vk0Wj
— Alex Berenson (@AlexBerenson) May 2, 2021
I was amused when I saw these Tweets to see Berenson use a term like “off-target effects” as if he actually knows what it means.
It turns out that this study on a preprint server has been published in Circulation Research. It also turns out—surprise! surprise!—to definitely not to be “smoking gun” evidence for Berenson’s claims. Unlike the case of many papers cherry picked by antivaxxers to support their claims, it’s not that the paper is horrible, either. It’s not. It’s pretty decent, actually, at least as a preliminary, primarily observational study. Even more amusing, in it the authors expressly describe how their work actually demonstrates why vaccines that use spike protein as the antigen are so effective, and the Salk Institute press release even includes a disclaimer that the spike proteins made in cells by SARS-CoV-2 “behave very differently than those safely encoded by vaccines”.
Let’s look at the paper itself. The first thing that those of you with access to the paper will notice is how short it is: Three pages, one figure. That’s because it’s not a full research paper, but rather a research letter. As a result, there’s no detailed Methods section, and the results are very briefly described (much too briefly, for my liking). To be honest, for some of the experiments, due to the brevity of the paper, I had a bit of a hard time making heads or tails of what, exactly, the investigators did. I’ll do my best trying to explain, however.
In brief, the researchers used a “pseudovirus” that was surrounded by a “crown” of spike protein, like the coronavirus, but did not contain actual virus, dubbed Pseu-Spike by the authors. What is a pseudovirus? A reasonable question. In brief, a pseudovirus is a construct that has the external proteins of the virus of interest. There are a variety of pseudoviruses now, as described in this article in The Scientist:
Among these, researchers turned to models of the pathogen such as pseudoviruses and chimeric viruses that can be studied safely in labs with lower biosafety level (BSL) clearance than required for studying the wildtype version, in an effort to expand the study of the novel coronavirus. Pseudoviruses don’t replicate, rendering them harmless, but by replacing their surface envelope proteins with those of SARS-CoV-2, researchers can glean insights into the ways the pathogen infects cells.
And:
Pseudoviruses were first developed in the 1960s, after scientists began studying a vesicular stomatitis virus (VSV) isolated from cattle. In addition to replicating well in culture, they later learned that its surface protein, VSV-G, facilitates entry into all eukaryotic cells, making the virus a useful vector not only as a pseudovirus but as a ferry to deliver DNA into cells for therapeutic purposes. The first Ebola vaccine was developed using a VSV platform, and more recently, the virus has been engineered to seek out and destroy cancer cells.
HIV-based platforms, which came about in the 1980s, have since replaced VSV as the most common model for developing both pseudo- and chimeric viruses. Unlike VSV’s negative-strand RNA genome that must be transcribed once inside the cell, HIV’s positive-strand RNA genome can instantly begin translation, making pseudoviruses based on HIV faster to produce. HIV-based model viruses have now been used in many of the same applications as VSV, with scientists applying them to the study of diseases such as AIDS, SARS, MERS, and influenza.
Also, compared with natural virus, a pseudovirus can only infect cells in a single round, has broad host range, high titer, and is not easily inactivated by serum complement.
Unfortunately, it is not clear from the paper which of these platforms was used to produce the pseudovirus in the experiments or how that pseudovirus was developed and produced. This is the sort of information that a full-length research paper would describe in the Methods section and it’s important information for determining whether the pseudovirus used was likely to be a good model. In another issue with this paper, the authors also do not describe the “mock virus” that they used as a control or how it was constructed. As a result, I find it very difficult to interpret their results. In fairness, some of this confusion might be because I am not highly knowledgeable about this particular system and don’t have the background knowledge about methodology that the authors clearly assume that the reader possesses. On the other hand, in a paper this in a journal like Circulation Research, which is not a virology journal, and particularly given that this is a paper that was likely to make the news and be misused by antivaxxers after its release, explanatory details that allow scientists from other fields with knowledge of molecular biology (but who are not experts in this field) to understand what was done are critical. A Research Letter does not accomplish this.
My concerns aside, let’s look at the experiments. The authors took pseudovirus or mock virus and instilled it into the tracheas of Syrian hamsters, three animals per experimental group. Another aspect of this study caught my eye, namely the amount of virus used, 5 x 108 pfu. For those of you not knowing what “pfu” stands for, it stands for “plaque-forming units.” Basically it’s a measure of the number of viable virus particles, virus particles that can infect cells and cause a plaque on a confluent layer of cells. That’s half a billion particles, far, far more of a viral challenge than the amount of virus launching any “natural” infection by SARs-CoV-2.
Using what is a highly artificial system, the authors compared the levels of a whole slate of protein markers related to cell signaling and oxidative stress in the mock- and Pseu-Spike-treated hamsters, as well as the histology of the lungs. I won’t go into detail about all of the markers examined, but rather will step back to take a longer view because it is not important for a lay person to understand all the phosphorylation of this protein or ubiquitination of that protein measured. (It’s also easy to get lost in the weeds of a study like this.) As stated, the authors found signs of inflammation in the alveoli (air sacs) of the Pseu-Spike-treated lungs, including thickened walls and inflammatory cells. They measured the levels of various proteins they deemed relevant:
AMPK (AMP-activated protein kinase) phosphorylates ACE2 Ser-680, MDM2 (murine double minute 2) ubiquitinates ACE2 Lys-788, and crosstalk between AMPK and MDM2 determines the ACE2 level.4 In the damaged lungs, levels of pAMPK (phospho-AMPK), pACE2 (phospho-ACE2), and ACE2 decreased but those of MDM2 increased (Figure [B], i). Furthermore, complementary increased and decreased phosphorylation of eNOS (endothelial NO synthase) Thr-494 and Ser-1176 indicated impaired eNOS activity. These changes of pACE2, ACE2, MDM2 expression, and AMPK activity in endothelium were recapitulated by in vitro experiments using pulmonary arterial ECs infected with Pseu-Spike which was rescued by treatment with N-acetyl-L-cysteine, a reactive oxygen species inhibitor (Figure [B], ii).
Translation: Compared to mock virus, Pseu-Spike altered signaling due to the ACE2 receptor, which is not surprising given that it’s been known for a year now that spike protein latches onto the ACE2 receptor in order to get SARS-CoV-2 into the cell. As a result, there was a lower level of ACE2 in the hamster lung tissue treated with Pseu-Spike, although looking at the Western blots in Figure 1B I am not particularly impressed by the magnitude of the decrease in protein level.
Also observed in the Pseu-Spike-treated hamster lung was decreased activity of eNOS, an enzyme that generates nitric oxide, as well as damage to the mitochondria, the “power plants” of the cell. The authors also did the same experiments in cell culture alone using pulmonary vascular endothelial cells (the cells the line the inside of the arteries in the lung), reporting that they recapitulated their findings, although they used spike protein at a rather high concentration (4 μg/ml). They also tested whether similar changes occurred in vascular endothelial cells genetically engineered to make a more stable and less stable version of ACE2. They did, although this is only suggestive, not slam dunk evidence, that it is the spike protein-induced degradation of ACE2 that results in these intracellular changes. The authors also reported that in pulmonary arteries isolated from the hamsters vasodilation induced by a drug called nitroprusside was not affected by Pseu-Spike, but the vasodilation caused by acetylcholine was impaired. Nitroprusside works by breaking down in the presence of oxyhemoglobin to produce, among other things, nitric oxide, while acetylcholine binds to specific protein receptors on the cell surface.
To be honest, I’ve never been a fan of papers this short (e.g., some Nature or Science papers, which can be even shorter than this) because I can never quite figure out what the authors did; this is one of the rare cases of a paper that to me screams out for an online Supplemental Data and Supplemental Figures section, and I say this as someone who generally detests the trend in scientific publications to dump all sorts of data into supplemental sections.
Let’s, for the sake of argument, take the results at face value and assume that this study shows what the authors say it shows, namely that spike protein damages endothelium, “manifested by impaired mitochondrial function and eNOS activity”. and can cause oxidative stress that destabilizes the ACE2 receptor, leading to lower levels of the receptor. The authors themselves note that by decreasing the level of ACE2, spike protein could actually decrease the infectivity of SARs-CoV-2, given that the coronavirus needs to bind to ACE2 to get into cells, while speculating that the dysfunction of endothelial cells could result in endotheliitis, or inflammation of the endothelium that more than makes up for the decreased infectivity.
But here’s the kicker, taken right from the final paragraph of the paper:
Collectively, our results suggest that the S protein-exerted EC damage overrides the decreased virus infectivity. This conclusion suggests that vaccination-generated antibody and/or exogenous antibody against S protein not only protects the host from SARS-CoV-2 infectivity but also inhibits S protein imposed endothelial injury.
In other words, the vaccine could be protective not just against infection by SARS-CoV-2 but also against endothelial injury from the spike protein.
I just want to reiterate again that this is a contrived system. It’s far from a worthless system, as pseudovirus systems have value in studying the role of spike protein in the pathogenesis of COVID-19. However, given the crapton of pseudovirus used in this hamster model, I really question any relevance of this system to vaccine safety issues with respect to mRNA- or adenovirus-based vaccines that produce the spike protein as an antigen. Why? The mRNA or adenovirus from the vaccines does not distribute extensively given that it’s an intramuscular injection, and the spike protein is highly unlikely to attain concentrations in the circulation anywhere near the high levels produced by the model used in these experiments. Moreover, the spike protein from the vaccine is not attached in a crown-like array on a virus particle (or pseudovirus particle), but rather exists as naked single protein molecules, and, as has been described before, it’s unclear that in this form spike protein, compared to the “crown of spikes” that gives coronaviruses their name, is anywhere near as effective at causing these downstream effects in cells. Add to that the fact that mRNA, even the modified mRNA in the vaccine, doesn’t hang around very long and therefore doesn’t generate spike protein for very long. (Doubters should consider this: Why do the mRNA vaccines both require a second dose 3-4 weeks after the first dose if, as many antivaxxers claim, the vaccines crank out spike protein indefinitely?)
Indeed, one of the authors pointed out this very issue and took antivaxxers to task for misusing their study:
i’m going to give a full response asap. but quickly for the record:
1) the (relatively) small amount of spike protein produced by the mRNA vaccine would not be nearly enough to do any damage
2) i happily got the mRNA vaccine, FWIW
3) i encourage everyone to get it— Uri Manor 💔 (@manorlaboratory) May 2, 2021
a couple prelim responses to anti-vaxxers misrepresenting these findings (here: https://t.co/qMhHyNyRR1). tl;dr: mRNA vaccine is waaaaay safer than COVID19 and everyone should get it – I did and everyone in my family did as well! Our paper just shows this disease really sucks. https://t.co/1t6SuUXZ5B
— Uri Manor 💔 (@manorlaboratory) May 2, 2021
Since I first discovered this study, it’s just amused me how obvious it is that the antivaxxers citing this study have obviously not actually read the study itself, nor have they considered the background science and knowledge behind the study. They’ve just read the press release. What do you expect, though? They’re antivaxxers. This study by Uri Manor’s laboratory is interesting and potentially important because it begins to elucidate the role of the spike protein itself in the pathophysiology of SARS-CoV-2 infection and how the spike protein alone can cause damage, but it does not in any way suggest that spike protein made by a COVID-19 vaccine is in any way toxic at the concentrations it’s produced, much less that it’s in any way “shed” or that the “shed” spike protein can cause disease or miscarriages in the unvaccinated who encounter the vaccinated.
Which brings me to the last of the three studies, which was published late last week.
The deadly coronavirus spike protein produced by the Moderna COVID-19 vaccine?
On Friday, I started seeing a study popping up among antivaxxers. Unsurprisingly, the “pandemic’s wrongest man” was all over it on Friday. His ability to misinterpret studies and thereby spread prodigious amounts of COVID-19 disinformation is depressingly impressive:
Hey, remember how all the smart people told you the vaccines were supery-dupery safe because those nasty-ass (technical term) spike proteins they make would never actually leave the cells that make them?
Turns out that's… less than entirely accurate.https://t.co/JJKdmOB4fU
— Alex Berenson (@AlexBerenson) May 21, 2021
The study itself was published on May 20 in Clinical Infectious Diseases, the official journal of the Infectious Diseases Society of America (IDSA) as a brief report by Ogata et al, entitled “Circulating SARS-CoV-2 Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients” and is the result of a collaboration between investigators at Harvard and the University of Montreal.
The study was very straightforward in design. In brief, investigators longitudinally studied blood samples from 13 participants who received two doses of mRNA-1273 (i.e., took samples at various time points after vaccination), Moderna’s mRNA-based COVID-19 vaccine. I can sum up the findings from the abstract, namely that investigators were able to detect spike protein in the plasma of 11 of 13 participants in the trial as early as one day after vaccination. To do so, they used a very sensitive technique known as single molecule array (SIMOA) to detect intact spike protein and its S1 fragment produced by RNA-1273.
A brief discussion of the spike protein itself is in order. The spike (S) glycoprotein of SARS-CoV-2 binds angiotensin-converting enzyme-2 (ACE2) on host cells. Spike itself is processed by proteases (protein-cleaving enzymes) into S1 and S2 subunits that remain associated with each other. Upon binding to ACE2 by the spike protein, the protein changes conformation that leads to S1 shedding and the cleavage of S2 by host proteases. You don’t really need to know the details for purposes of understanding this study, other than that spike protein has an S1 and S2 subunit, and these subunits associate with each other in the same conformation as they were before protease cleavage. This is a diagram of the structure.
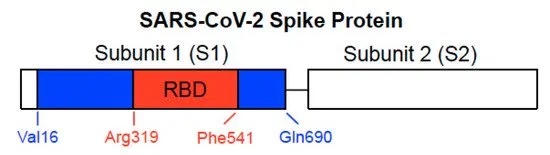
SARS-CoV-2 spike protein structure.
But what does the authors’ finding of spike protein in the plasma mean, if anything? Haven’t we always been reassured that the spike protein from the mRNA vaccines doesn’t get into the bloodstream and remains in cells and on the surface of the cells that produce the protein after vaccination? Isn’t this study, as antivaxxers like Berenson claim, a reason to be afraid of the Moderna vaccine, at least? The short answer to that last question is no. The longer answer follows.
We at SBM like to repeat Paracelus’ famous dictum, dosis sola facit venenum, or “only the dose makes the poison”. It’s a general principle of pharmacology and toxicology, namely that the dose determines the effect of a drug, or, more specifically, the concentration of any substance in the bloodstream or organs that it affects (which is related, of course, to the dose) is what matters in terms of its effects. As I like to say, even water can be toxic if too much is ingested. That’s why I’ll refer back to a common antivaccine trope for which I long ago coined a term, “the toxins gambit“. Pre-pandemic, antivaxxers would point to every scary-sounding chemical they could find in vaccines and try to use it as evidence that vaccines were laden with “toxins”. My favorite example is, of course, formaldehyde, which is used in the preparation of some vaccines in order to inactivate the virus used as an antigen, leaving detectable traces behind in the vaccines. I first discovered the “formaldehyde gambit” (a form of the “toxins gambit”) when it was used years ago by Dr. Jay Gordon. The short version of the refutation of the “formaldehyde gambit” is to cite Paracelus and point out that the amount of formaldehyde in any given vaccine is exceedingly small, considerably smaller than what an infant produces due to their own normal metabolism. Indeed, peak body burden of formaldehyde has been estimated to be less than 1% of endogenous formaldehyde.
The same thing applies to this study cited by Berenson, as you will see. Before I describe how much spike protein the investigators found in the plasma of these 13 study participants, let’s look at the concentrations used, for example, in the cell culture experiments done by Uri Manor’s group as described in the second paper I discussed: 4 μg/ml.
Now, let’s look at the “money figure” from the paper, the first three panels of Figure 1. The reason that the authors also did the assay to detect the viral nucleocapsid protein was because the vaccine does not result in production of this protein. It was thus a negative control; unless the subject is infected with SARS-CoV-2, nucleocapsid protein should be undetectable.
Here’s the figure:
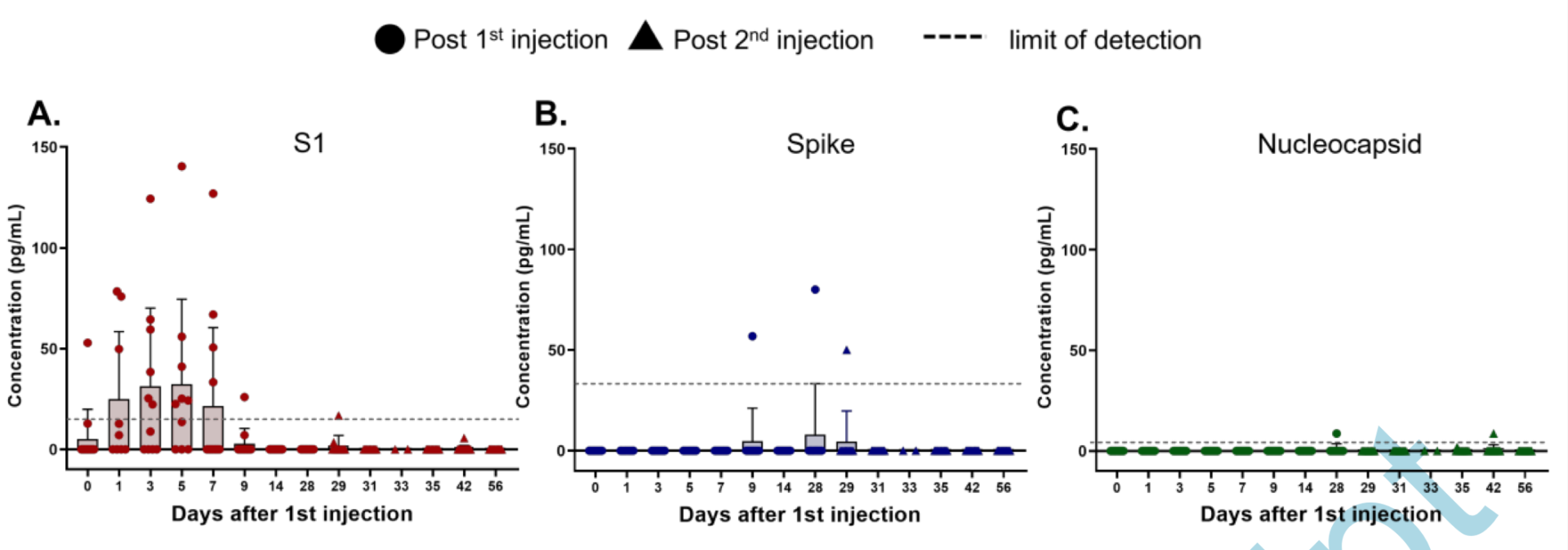
Spike protein after vaccination with Moderna RNA-1273. Note the Y-axis units.
Now take a look at the Y-axis, in particular, the units on the Y-axis: “pg/ml,” or picograms per ml. That’s 10-12 grams/milliliter. What was the concentration used by Manor’s lab again? Oh, yes, 4 micrograms/milliliter. One microgram is 10-6 grams, or one million-fold more than one picogram! Or, as Uri Manor put it:
Congrats to @OgataAlana on this important study. Many asked how much spike protein gets into circulation after vaccination. Turns out to average ~30-40 pg/mL for a few days then disappears.
FYI: This is ~100,000x less than used in our paper (4 ug/mL).https://t.co/k5AChClhI5 pic.twitter.com/xgzJ4RerYG
— Uri Manor 💔 (@manorlaboratory) May 21, 2021
Or, as Ogata et al write:
S1 antigen was detected as early as day one post vaccination and peak levels were detected on average five days after the first injection (Figure 1A). The mean S1 peak levels was 68 pg/mL ±21 pg/mL. S1 in all participants declined and became undetectable by day 14. No antigen was detected at day zero for 12 of 13 participants, as expected. However, one individual presented detectable S1 on day zero, possibly due to assay cross reactivity with other human coronaviruses or asymptomatic infection at the time of vaccination. Spike protein was detectable in three of 13 participants an average of 15 days after the first injection. The mean spike peak level was 62 pg/mL ± 13 pg/mL. After the second vaccine dose, no S1 or spike was detectable, and both antigens remained undetectable through day 56. For one individual (Participant #8), spike was detected at day 29, one day after the second injection and was undetectable two days later.
Let’s be generous. Let’s look at panel B and examine the highest concentration of spike protein detected, which looks by the graph to have been around 90 pg/ml. Now, for ease of calculation, let’s just round up to 100 pg/ml as the highest average peak plasma concentration of spike protein after vaccination. That would still be a 40,000-fold lower concentration than 4 μg/ml. As an aside, the authors also detected IgG and IgA antibodies to spike protein and a correlation between clearance of detectable SARS-CoV-2 protein and the production of IgG and IgA.
But why did Ogata et al detect any spike protein at all? After all, we know that the spike protein is not secreted from the cells in which it is made because it lacks an amino acid sequence, a so called “signal peptide sequence” that would lead to its secretion. We know that the spike protein as made using the mRNA sequence template is membrane-bound, meaning that it’s embedded in the membrane of the cells that make it. The authors speculate in the Discussion:
In this study, 11 participants exhibit S1 antigen in plasma after the first injection, while nucleocapsid concentrations are insignificant in all participants, confirming that the detected S1 originates from vaccination and not natural infection. The presence of S1 is likely due to the nature of the encoded mRNA-1273 spike protein, which contains a cleavable S1-S2 site and enables release of S1 from the spike trimer2. We hypothesize that release of S1 protein could result from cleavage via mammalian cell proteases or circulating proteases. We observe an increase in S1 over an initial period of one to five days, suggesting that mRNA translation begins immediately after vaccine inoculation. Interestingly, spike protein appears in three of thirteen participants on average eight days after S1 is produced.
Translation: There are enzymes that can cleave proteins (proteases), and it is possible that these proteases clipped off the S1 subunit from the spike proteins in the membrane.
Another possibility:
The Simoa antigen assays for the full spike protein are designed to require antibody binding to both the S1 and S2 subunits for detection, resulting in a cleaved spike protein to be undetectable. Additionally, spike protein concentrations in plasma of vaccinated participants may be below our assay limit of detection. We hypothesize that the cellular immune responses triggered by T-cell activation, which would occur days after the vaccination, lead to direct killing of cells presenting spike protein and an additional release of spike into the blood stream. The mechanisms underlying release of free S1 and the subsequent detection of the intact spike protein remain unclear and require further studies.
In other words, another possibility is that the immune system killing the cells producing spike protein could result in the release of enough spike protein to be detectable by this very sensitive assay. Indeed, the authors note that the detection of spike protein “has not yet been described in any vaccine study, likely due to limitations in assay sensitivity and timing assessment”. In other words, the authors’ assay is so sensitive that it’s detecting incredibly minute amounts of spike protein from the vaccine in the blood that previous studies could not detect, simply because they used insufficiently sensitive assays.
As I was writing this, I was informed that an old friend Ed Nirenberg had done a similar analysis and had actually done me one better by comparing this study to another study of spike protein that reported that spike protein could damage the blood-brain barrier. That study used a 10 nM (nanomolar) concentration of spike protein, which, using the molecular weight of spike protein and S1 subunit and found:
A 10 nM solution of these [spike protein and S1 subunit] would equate to 14,610,000 pg/mL and 7,650,000 pg/mL respectively which are respectively 146100 times and 76500 times more spike protein than is found in plasma of vaccinated people.
Ed further notes:
Ah but I hear you protesting- the experts lied! They said no spike circulating- clearly there’s spike circulating. Not exactly. For one thing, the data available until this point didn’t show evidence of spike circulating, and we have a tendency in shorthand to say that that means there is no spike because we can’t prove a negative. All assays have limits of detection (in this case it’s labelled). A 10 nM concentration is very small- and yet this is still about 100,000 times more spike than what we find in plasma. This assay is pretty special to be able to find anything reliably at this concentration and I would be skeptical of its accuracy at this level if not for the time points that these things are appearing. Also note that this isn’t evidence of spike protein being secreted by the cells that receive the mRNA, which was the key consideration behind such claims and indeed based on the tiny quantities noted, that doesn’t appear to be happening. The appearance of intact spike in the plasma of this admittedly small sample is very rare and transient.
Exactly. The amount of spike protein that was detected by SIMOA in this study is low, basically not much above the current limit of detection for this protein, and, more importantly, very transient. There was nothing nefarious in previous statements that spike protein from vaccines does not circulate in the bloodstream, nor was it a lie. Again, to echo Ed, the key concern was that the cells that took up the lipid nanoparticles containing the mRNA should not secrete the spike protein product, which could, theoretically at least, actually produce a significant plasma concentration.
On Twitter, Alana Olgata notes that she’d like to repeat this study with other COVID-19 vaccines, which is not unreasonable:
Yes. Completely agreed. Our goal to repeat these studies with other vaccines, especially J&J and OAZ. The challenge now is acquiring these samples as the vaccine roll out slows down and with high frequency sampling.
— Alana Ogata (@OgataAlana) May 21, 2021
No doubt antivaxxers will leap all over those papers when they are published.
The “deadly” spike protein and vaccine safety
As I stated near the beginning of this post, antivaxxers strive mightily, above all, to claim that vaccines are dangerous to those receiving them and those around the recipients, all with added conspiracy theories. It doesn’t matter how much they have to misinterpret or misrepresent scientific studies to do so. They’ll find a way to make their misrepresentations (or failure to put studies into proper context) sound like plausible evidence that vaccines are dangerous, and they’ve certainly been doing this with COVID-19 vaccines, starting with pointing to any study that finds a role for the spike protein alone in causing cell damage. Such studies are critical to the elucidation of the molecular mechanism by which SARS-CoV-2 infects cells, replicates itself, and causes so much damage to the lungs. It’s also important to note that target effects matter. Location matters. The main infection starts in the lungs, which is where the highest concentration of virus and therefore spike protein would be expected in the case of real infections. In the case of vaccination, the location is the muscle cells of the shoulder, and any spike protein that escapes is rapidly diluted in the bloodstream to the pg/ml range.
But what does Olgata’s finding for the Moderna mean regarding the safety of the vaccine? Basically nothing. The reason is simple. If there were a safety problem due to spike protein, after more than a quarter of a billion doses of vaccine administered in the US alone, there would have been safety signal by now, given the unprecedentedly intense vaccine safety surveillance effort that accompanied the rollout of these vaccines. Remember, this is a pharmacosurveillance effort that detected literally a one-in-a-million serious adverse event associated with vaccination with the Johnson & Johnson vaccine within a month and a half of its being distributed under an emergency use authorization. It beggars the imagination to suggest that, even if the transient appearance of spike protein after vaccination at a concentration of (at most) tens of picograms/ml were toxic, there would be no safety signal after so many doses. It’s even more ridiculous to propose that such a minuscule concentration of spike protein can be “shed” in quantities that could affect other people, given the incredibly low and transient concentration produced after vaccination.
Antivaxxers either don’t know or understand that themselves, or they know that the vast majority of people don’t know or understand that. All they need is a finding that any spike protein floats free in the bloodstream after vaccination, and they can use that finding to start an effective fear mongering campaign. That’s exactly what they are doing now.