
{kind=link}
[Editor’s note: Due to a personal issue, Jann Bellamy was unable to write a post for today. As a result, I filled in. Some of you might have seen this before elsewhere, but I thought the topic was important enough to discuss here on SBM as well.]
I’ve described in the past many times how advocates of “integrative medicine” (or, as I like to call it, “integrating” quackery with conventional medicine) like to co-opt science-based treatments as somehow being solely within the bailiwick of their favored unholy hybrid medicine offspring bred of a forced marriage between science and magical thinking. There are many potentially harmful aspects of this shotgun marriage, not the least of which is the dilution of the scientific basis of medicine in favor of pseudoscience. One area, however, that doesn’t get enough attention (except from me) is how integrative medicine tries to claim all “nonpharmacologic treatments for pain” as its own. I’ve described how quacks have done this.
My thinking on this issue first started to gel a couple of years ago, when the National Center for Complementary and Integrative Health (NCCIH) published its five year strategic plan for 2016-2021. In this plan, NCCIH prominently featured researching and promoting the “nonpharmacologic treatment of pain” as one of its most pressing goals. Later that year, it published a really bad review article, one based on horrible studies and huge extrapolations from weak data, that basically claimed all nonpharmacological treatment of pain as part of “complementary and alternative medicine” (CAM, now known as “integrative medicine”). Basically, although I had been getting the vibe that integrative medicine advocates were trying to claim all non-drug treatments for pain as their own before this, these two publications by NCCIH made it incredibly obvious to me that this was the new propaganda direction that integrative medicine advocates would be taking, and take it they did. It wasn’t long before JAMA joined in, followed by the American College of Physicians, the Academic Consortium for Integrative Medicine and Health (of course!), and the FDA which, in response to lobbying by acupuncturists and chiropractors, has a draft proposal outstanding to encourage physician education about acupuncture and chiropractic as “therapies that might help patients avoid prescription opioids.” Never mind that there is no good evidence that either can accomplish this goal. Meanwhile, acupuncture advocates have been busy lobbying various states to have their Medicaid programs cover acupuncture.
Which brings us to Oregon.
Oregon: The “nonpharmacologic treatments for pain” scam
There was a story last month that I had meant to write about but somehow had gotten lost in the piles and piles of links in my “to be blogged folder” about the potential horrible consequences for patients that this co-optation of nonpharmacologic treatments for pain could have for chronic pain patients, in essence sanctioning their torture. (I don’t think I’m exaggerating, or if I am it’s not by much.) It came in the form of an AP story, “Oregon officials consider limiting opioid prescriptions“:
A proposed change to the state’s Medicaid program aims to reduce the overprescribing of opioids, which has caused an epidemic of overdoses, Oregon officials said.
The proposal would limit coverage for five broad chronic pain conditions to 90 days of opioid pain relievers, The Bulletin reported Wednesday.
It would also taper off patients who have been taking opioids long-term from those medications within a year.
In turn, it would introduce alternative treatments previously unavailable under the Oregon Health Plan.
“Alternative” you say? What does that mean? If you read this blog, I bet you know exactly what that means. From The Bulletin, a central Oregon newspaper:
Oregon could have some of the country’s strictest limits on opioids for chronic pain patients under a proposal being considered for the state’s Medicaid program. The proposed change would limit Oregon Health Plan coverage for five broad chronic pain conditions to 90 days of opioid pain relievers and would force patients who have been taking opioids for longer to be tapered off those medications within a year.
Yikes! Forced tapers for chronic pain patients beginning in 2020? What, pray tell, will replace the opioids? You guessed it: yoga, acupuncture, massage, chiropractic, or physical therapy. Or, as an Oregon Health Authority spokesperson put it:
“We are in an opioid crisis in Oregon,” said Jonathan Modie, an OHA spokesman. “Over prescribing has been the main driver of overdose and death. We want to make sure patients have more non-pharmacological options such as acupuncture, massage therapy and chiropractic care.”
Well, yes. There is an opioid crisis. Deaths due to opioid overdose are at an unacceptably high level. Something needs to be done. Unfortunately, the imperative to “do something, anything” is driving some truly awful policies that will harm patients. For example, in my state, as of June 1, physicians have to run a search on every patient for whom they prescribe opioids beyond a three day course for acute pain (as in postoperative prescriptions) and document that search on a special opioid prescription form. We also have to have patients sign a consent form warning them that opioids can be addictive and can even kill them. Will this policy reduce opioid overdoses in this state? Hell if I know! There’s no good evidence to say that it will, but it might just accomplish that by making it so onerous to prescribe and get opioids, even for patients who need them, that fewer patients get opioid prescriptions and therefore fewer die. The price, of course, is a lot of patients in pain who don’t need to be. Of course, the Oregon proposal is so much worse. At least the Michigan proposal has a little bit of prior probability based on callousness: Let patients suffer by making it harder for them to get opioids and maybe overdoses will decline. It might work if as a state official you don’t mind treating some chronic pain patients with needless cruelty. The Oregon proposal, on the other hand, can’t work because it proposes encouraging the use of quackery instead of opioids.
Now that’s cruel.
Three acupuncturists and a chiropractor
Where, you might wonder, did such an incredibly non-evidence-based and, to put it quite bluntly, dumb proposal come from? It takes a little explaining, explaining that’s easier to do just by quoting:
The proposed change came out of the Chronic Pain Task Force, an ad hoc committee created to provide guidance on reducing opioid use under the Oregon Health Plan. The Oregon Health Plan has a unique structure among state Medicaid programs, relying on a prioritized list of health services ranked by experts in order of importance to patients. State lawmakers then decide where in the prioritized list to draw the line between covered and uncovered services.
Currently, the five conditions being discussed — fibromyalgia, chronic pain syndrome, chronic pain due to trauma, other chronic postprocedural pain and other chronic pain — fall below the line, and thus treatments for those conditions aren’t covered by the Oregon Health Plan. But according to the Oregon Health Authority, many patients with those five conditions are being prescribed opioids. The Oregon Health Plan has no way of knowing whether those patients are being prescribed opioids for those chronic pain conditions or for covered services and, therefore, cannot decline to cover those prescriptions.
By establishing a new entry in the prioritized list above the cutoff line, the Oregon Health Plan would then cover alternative treatments, such as yoga, acupuncture or physical therapy, but would try limit the use of opioids.
I’m all for evidence-based guidelines for just about every condition in medicine with sufficient scientific and clinical evidence upon which to base guidelines, but the key is how these guidelines are developed. Using Google to try to find various reports of the Oregon Chronic Pain Task Force, I found this Health Evidence Reviews by the Chronic Pain Task Force dated January 23, 2018 and June 7, 2018. I could see the problem right away as I perused these documents. Basically, the problem was that the review of evidence listed in the reports tended to cite the same unconvincing studies that acupuncture and integrative medicine advocates like to cite. They cited follow-ups to the infamous Vickers meta-analysis (or, as I like to call them, Son of Vickers, Bride of Vickers, and the like), the granddaddy of acupuncture meta-analyses and the one most often touted as the gold standard “proving” that acupuncture works for chronic pain. It didn’t, no matter how much acupuncture advocates strained to say it did. Then, of course, the Task Force cited the systematic review by the NCCIH that really didn’t show that acupuncture or other CAM (rebranded as “nonpharmacologic treatments for pain”) has any effect on chronic pain distinguishable from placebo.
You can listen to the panel itself debating the opioid taper at its meeting of June 7. It’s cringe-inducing. They admit there’s no evidence, and basically admit that the figures they’re bandying about for length of time for the taper to zero have basically been pulled from their nether regions:
Notice the obsession with being consistent with the “prior guidelines”. What prior guidelines, you ask? Well, in 2016, Oregon imposed similar restrictions on patients with chronic back pain. At one point, they assert that this program is working, but there’s no evidence presented that it is, nor could I find any evidence that it’s doing what is intended. Basically, they want to expand their forced taper to a much larger group of patients.
It didn’t take me long to figure out why the Chronic Pain Task Force is so “open” to alternative treatments. There are three acupuncturists (Ben Marx, David Eisen, and Laura Ocker) and a chiropractor (Mitch Hass) on the committee. Yes, you read that right. Four of the members of the Oregon Chronic Pain Task Force are quacks. They’re cruel quacks, too, as they want to force patients to taper their opioids in favor of their fraudulent “nonpharmacologic treatments for pain”.
Ocker, for one, is a high-ranking and influential quack, too. She was President of the Oregon Association of Acupuncture and Oriental Medicine from 2012-2013 and has been active promoting acupuncture legislatively in Oregon at least since 2009. Indeed, our old friend John Weeks interviewed her admiringly in May 2017, claiming that “Evidence opens Medicaid in Oregon to acupuncture,” where we also learn that Ben Marx has been one of her colleagues at the Oregon College of Oriental Medicine also working to promote acupuncture reimbursement in Oregon:
Ocker has also made available multiple documents that can guide interested parties more deeply into how to engage such a process. These include the recent Oregon Health Plan remarkable decision, following the ascendency of the opioid crisis, to “prioritize therapies such as chiropractic and osteopathic manipulation, physical therapy, acupuncture, cognitive behavioral therapy, graded exercise therapy, interdisciplinary pain management, yoga, and massage—and a treatment plan to stay active and return to previous function—over ineffective surgeries and narcotics.” Ocker believes that the looming opioid crisis has been wind at their backs during the entire process.
In other words, at least two of the acupuncturists on the Chronic Pain Task Force are not just acupuncturists. They’re advocates for acupuncture and federal and state reimbursement for acupuncture services and have been active politically for quite some time working for just that. In addition, Amber Rose Dullea is a fibromyalgia sufferer and licensed massage therapist, as well as a “coach, speaker and author.
I couldn’t help but wonder: Are there any physicians on this task force? It turns out that there are. There are two anesthesiologists (Dr. David Sibell), one of whom is a pain specialist (Dr. Kevin Cuccaro). I must admit, after perusing Dr. Cuccaro’s website, I was left with the distinct impression of woo, as I read of the “Pain Triangle”. At the very least, his publications and podcast go on about the “Pain Management Business–A multi-billion dollar empire motivated by what is profitable rather than what is best for patients”. In episode #39 of his podcast, he starts right out going on and on about the “powerful placebo,” a dead giveaway for someone whose mind is so open that his brain falls out when it comes to woo. After all, placebo effects figure prominently in the central dogma of alternative medicine. The others include a fairly unremarkable assortment of specialties, including Dr. Tracy Muday, Chief Medical Officer of Southwest Oregon Independent Practice Association and Advanced Health, Coordinated Care Organization administering Oregon Health Plan benefits to enrollees in Coos and Curry counties; Dr. Holly Jo Hodges, Medical Director at WVP Health Authority; and Dr. Ariel Smits, a family medicine doctor in Portland.
It certainly looks as though the doctors barely outnumber the quacks on this panel, and might even have the upper hand. Why is this panel like this? An Oregon Health Authority spokeswoman justified it by saying that the task force composition aimed “to represent the variety of clinicians who would be involved in the management of chronic pain.”
Here’s the actual text and the changes from previous policy on the use of opioids for chronic back pain from 2016 (yes, that was the precursor to this cursed policy):
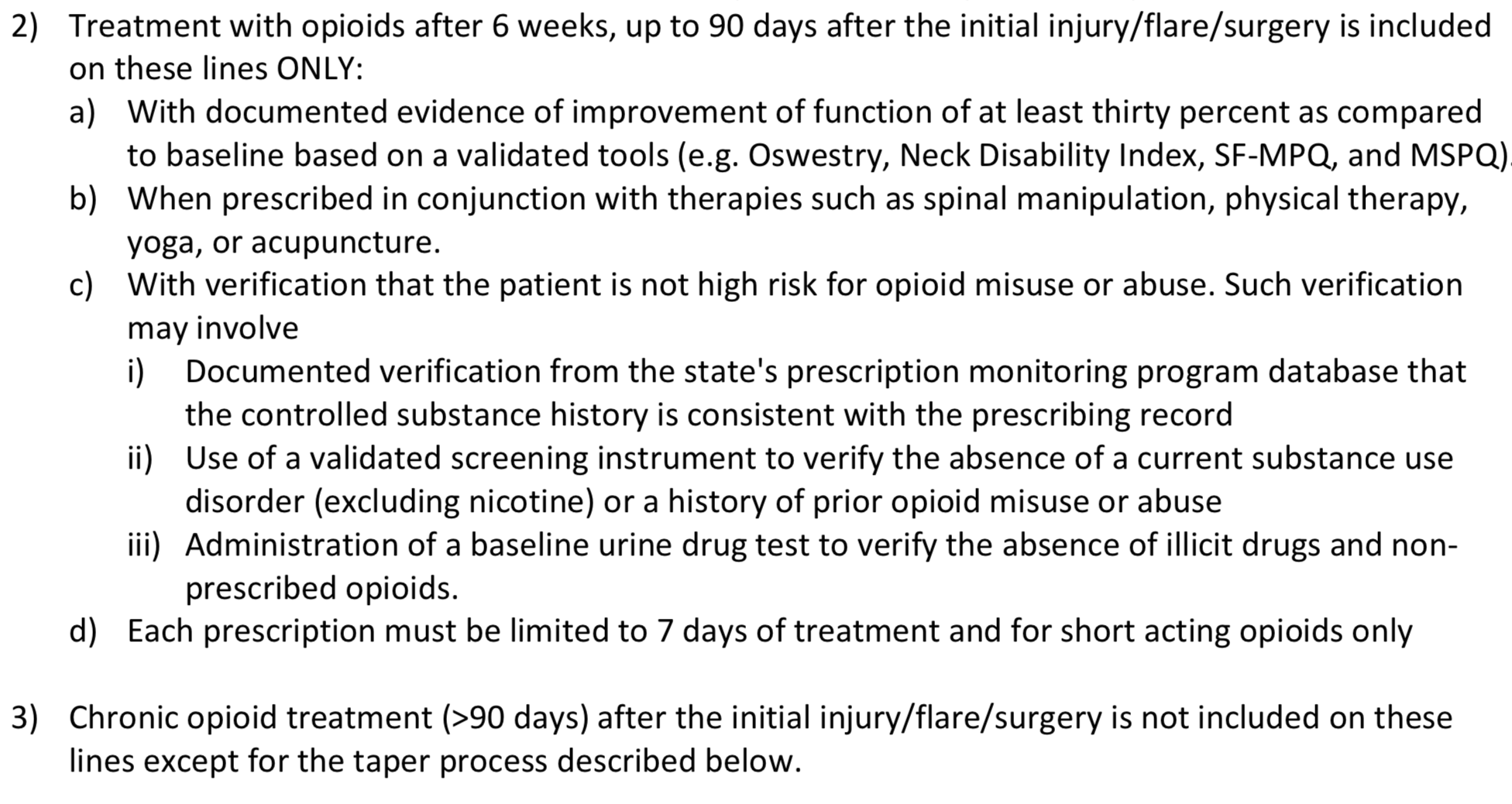
And what is this taper process? This:
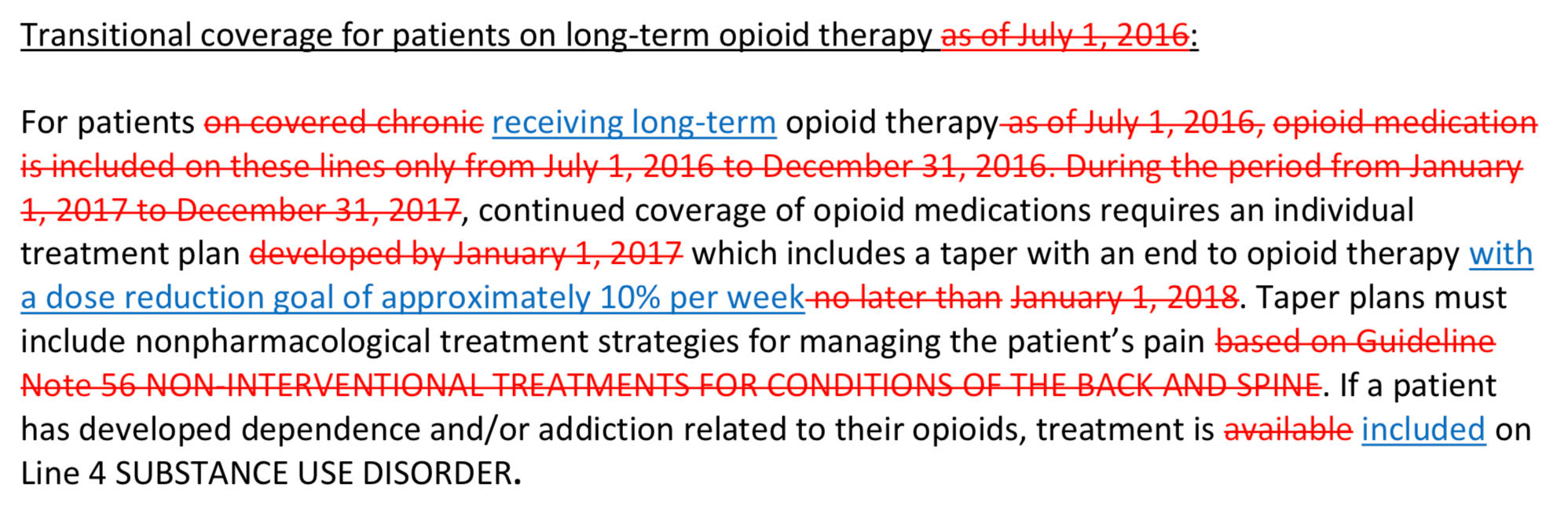
My reaction: WTF?
The backlash
Not surprisingly, groups representing chronic pain patients are not happy about these proposed guidelines. A story in STAT News from last week described how patients in Oregon are protesting, having shown up to an August 9 meeting of the Value based Benefits Subcommittee (VbBS) and the Health Evidence Review Commission (the latter of which includes a naturopath, Angela Senders, as one of its members) to make their concerns known, especially since the HERC is the committee that has to vote on the proposal, after it’s screened and approved by the VbBS. And, boy, did they ever!
The controversy has brought together an unlikely crew of protestors, including many in wheelchairs and in walkers, who, at 7:15 on a recent Thursday morning, erected a tidy encampment outside the windows of a community college lecture hall here. A security guard eyed them warily from inside, where an obscure committee would soon hear the state’s proposal to end coverage of opioids for chronic pain.
Among their signs: “Death with dignity is a law: What about LIFE with dignity?”
And:
Each used their time in the lecture hall to offer impassioned speeches, accented alternately with tears, shouts, shakes of a pill bottle, uniformly opposing the policy change.
Again and again, they reminded the committee members that they had not yet fully grappled with the question central to their proposal: Is continued reliance on opioids for chronic pain more dangerous than forcing patients off them?
And that’s the point:
Experts say the science supporting either argument is extremely limited.
“What is notably missing is any review of any literature regarding the centerpiece of their proposed policy: Forced opioid taper to zero for all persons,” said Dr. Stefan Kertesz, a pain and addiction specialist at the University of Alabama, Birmingham, School of Medicine.
Indeed, a group of pain physicians, academics, and patient advocates wrote a letter to Oregon Health officials pointing out just how wrong-headed and harmful this proposal is. The full text of the letter can be found here, but a key quote is worthy of noting:
An across-the-board denial of opioid therapy for the huge umbrella category of chronic pain is as destructive as is liberally prescribing opioids for all types of chronic pain,” the letter warns. “The denial of coverage to the Medicaid population, in particular, is likely to have a disproportionate impact on individuals with disabilities, on the sickest patients and those with multiple chronic conditions.”
Precisely. They also note that, although opioid prescribing has been declining since 2012, that decline has not correlated with a decline in opioid overdose deaths. Indeed, the authors note that opioid deaths have skyrocketed during that same period because “crisis has evolved to feature heroin and illicitly manufactured fentanyl and its analogs” and even “most deaths that involve a prescription opioid are polypharmacy—often including illicit drugs, benzodiazepines and other CNS depressants, and alcohol—and most misuse is non-medical.”
The danger of “integrating” quackery into medicine
Let’s just put it this way. Even “integrative medicine” pain specialists were appalled. The Academy of Integrative Pain Management submitted a statement. While the statement lauds the intent to make acupuncture and chiropractic (as well as other non-evidence-based treatments) “above the line” and thus reimbursable, even “integrative medicine” practitioners were horrified at the thought of forced opioid tapers. The statement also sarcastically notes Oregon’s first foray into this sort of nonsense by pointing out that it’s “in the 20th month of a similar 12-month plan to forcibly taper patients with back and spine pain off their opioid pain relievers” and then goes on to point out that this policy “is not a rousing success, yet you appear to be willing to impose it on another large group of patients.”
This proposal by the Chronic Pain Task Force in Oregon is also incredibly unethical. The reasons are simple. There is no evidence that forced opioid tapers—particularly a forced taper to zero opioids—is of any benefit for chronic pain patients, but there is considerable anecdotal evidence of potential harms, up to and including suicide. Indeed, Department of Veterans Affairs data suggests that opioid discontinuation is not associated with overdose mortality but is associated with increased suicide mortality. Moreover, denial of coverage for opioids in these patient groups will almost certainly have a disproportionate impact on patients with disabilities, on the sickest patients and those with multiple chronic conditions. These are the patients who frequently wind up on Medicaid after they can no longer work. Worse, the evidence that the modalities that will be covered and will be recommended as replacements for opioids are effective is weak to nonexistent. Indeed, the highest quality evidence shows that acupuncture, for instance, is no more than a theatrical placebo. It does not work.
If you want to see the danger of “integrating” quackery with medicine, as integrative medicine does, look no further than Oregon. Here, because of the way that integrative medicine has so successfully rebranded quackery like acupuncture as “nonpharmacologic treatments for pain” and tarted them up as being evidence based when they are not, a large state is seriously considering a policy that, if implemented, would leave an large number of the most vulnerable patients suffering unnecessarily, all because there are four quacks and at least some quack-sympathetic doctors and advocates on a panel. The opioid crisis is truly driving not just bad solutions born out of the desire to “do something”, but is being used as a “wedge” to drive more pseudoscience into medicine. Unfortunately, the fix seems to be in. There’s going to be a vote as early as October, and I’d be willing to bet—sadly—that Oregon will approve this patient-hostile policy. Then, moralizing about those who need opioids combined with magical thinking like acupuncture will leave untold patients suffering unnecessarily—all because we have to “do something”.
Don’t say I didn’t warn you this was coming somewhere, sometime. I also predict that, if Oregon gets away with this, it won’t be long before more states decide to punish chronic pain patients in the name of helping them with “nonpharmacologic treatments for pain.